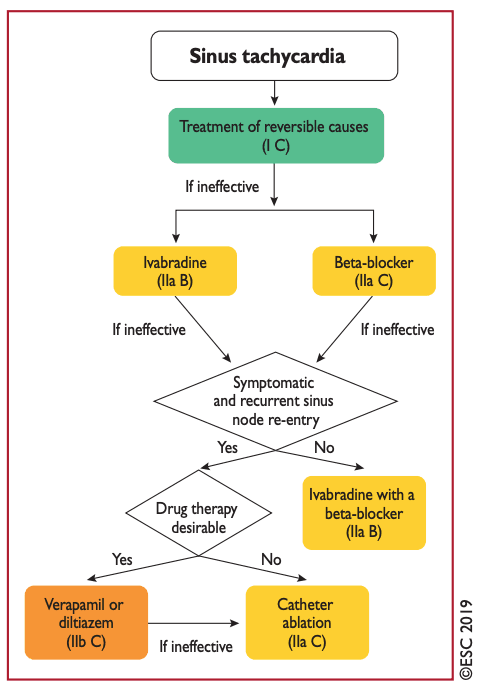
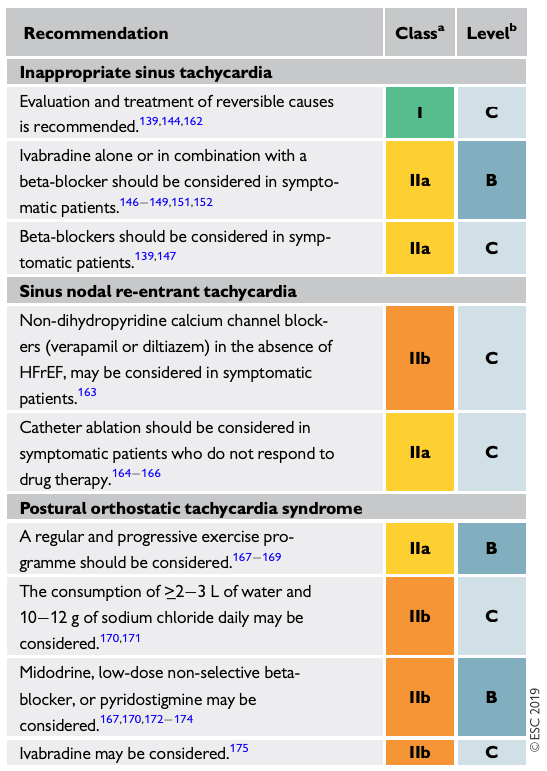
Sinus Tachycardia Introduction Mechanism: Increased automaticity of the SA nodeDefined as sinus rate > 100 bpm Response to Adenosine Gradual slowing of the tachycardia and then re-accelerationSinus nodal re-entry tachycardia will suddenly terminate ECG Characteristics Gradual onset & offset (driven largely by the autonomic nervous system)P-wave morphologyMatches P-waves in sinus rhythmPositive in I, II, aVF, and biphasic/negative in V1 [Should originate in the SVC-RA junction]Presence of conditions that drives sinus tachycardia: i.e. pregnancy, effort, stress Sinus Tachycardia: Note gradual acceleration and positive P-waves in lead II Management Must exclude POTs, sinus re-entrant tachycardia, focal AT from superior crista terminalis or RSPVSometimes need EPS to exclude sinus re-entrant tachycardiaThe following are diagnoses associated with sinus tachycardia:Physiologic sinus tachycardia (PST) Correct underlying cause, no specific therapy neededCommonly: Hypovolemia, Anemia, Hyperthyroidism, PE, PheochromocytomaInappropriate Sinus Tachycardia (IST) >100bpm at rest or minimal activity (out of proportion) – generally young female.Holter – mean HR > 90bpm, exaggerated > 100bpm during waking hrs.Prognosis benign, not associated with tachycardia cardiomyopathyTherapy:1st Line: Lifestyle: exercise training, volume expansion, avoid stimulants2nd line:B-Blockers (high doses needed) orIvabradine (usually with B-blocker to avoid paradoxical sympathetic increase)Sinus Node Re-entrant Tachycardia (SNRT)Re-entry circuit involving the sinus nodeUnlike IST, these are paroxysmal episodesDrugs:B-Blockers are often ineffective1st line: Verapamil/Diltiazem (IIB), avoid in HFrEFCan try amiodarone2nd Line: Catheter ablation if do not respond to drugs (IIA) ESC 2019 Guideline: Management of sinus tachycardia ESC 2019: Sinus Tachycardia POTSHR ≥ 30bpm when standing > 30s (or ≥ 40bpm in 12-19yo) [Usually females 12-19yo]ABSENCE of orthostatic hypotension50% spontaneously recover in 1-3yrsMany mechanisms describedNon-Pharmacologic:Increase salt/fluid intake, increase blood volume (10-12 g/day salt, ≥2-3L/day) (IIB)Exercise program (start with non-upright like rowing) (IIA)Pharmacologic:Midodrine TID daytime (IIB)Propranolol 10-20mg (non-selective BB ideal to block Beta-2 receptor) (IIB)Ivabradine (with BB) can be considered (IIB) References:ESC 2019 Guidelines for the management of patients with supraventricular tachycaria <- Back to Narrow QRS Tachycardia Page Post author:Pavel Antiperovitch Post published:April 2, 2020 Post category:Arrhythmia and Devices / Cardio Topics / Uncategorized