Acute Heart Failure (AHF) is worsening or decompensation of the signs and symptoms of heart failure
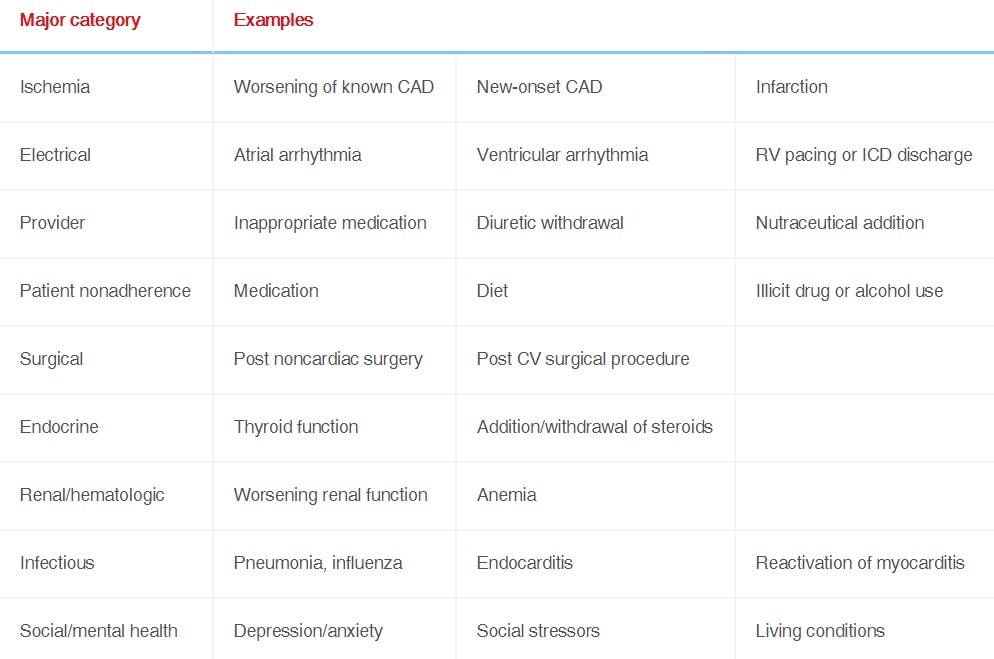
Initial evaluation should focus on confirming diagnosis and precipitating causes
Treatment includes supportive measures (i.e. oxygenation and blood pressure), loop diuretics for volume overload, and escalating advanced therapies if required
Once out of the acute phase, guideline-directed medical therapy should be initiated (discussed in the Chronic Heart Failure topic)
Diagnosis
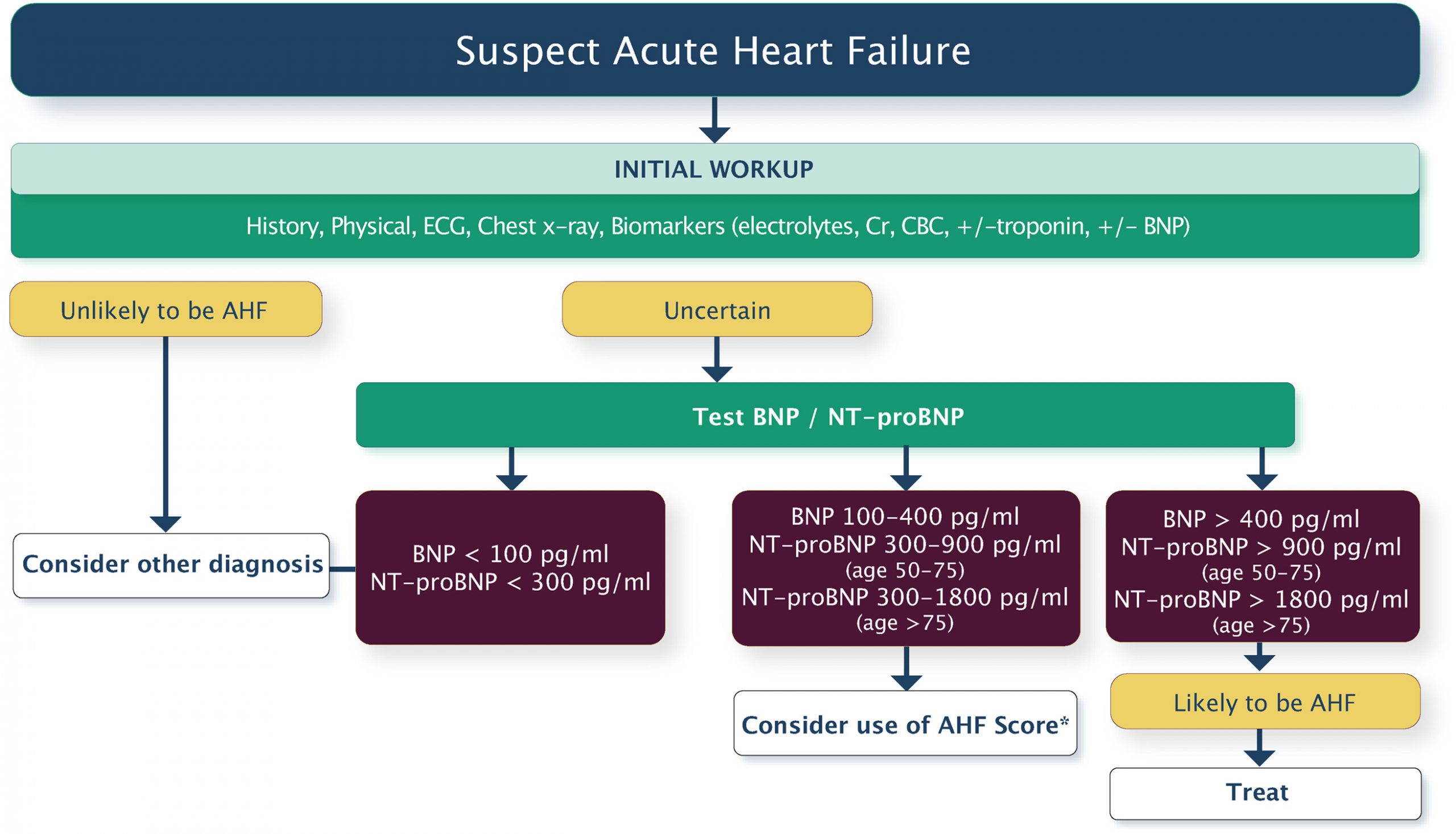
CCS Diagnosis Algorithm
CCS Diagnosis of heart failure in the acute care setting.
BNP (use to increase/decrease pretest probability, follow treatment, and as a prognostic marker)
Troponin (use to assess for ischemia, and to prognosticate – persistently elevated Tn is a marker of poor prognosis)
Imaging:
CXR (cardiac size, congestion, and other pulmonary processes)
ECG (arrhythmia, ischemia, and structural abnormalities)
Transthoracic echo*
Any other investigations required to workup precipitant and cause of heart failure
*Perform within 72 hours of admission. If previous echo < 12 months ago, no significant change in clinical status, and responding to therapy do not need to repeat.
Treatment
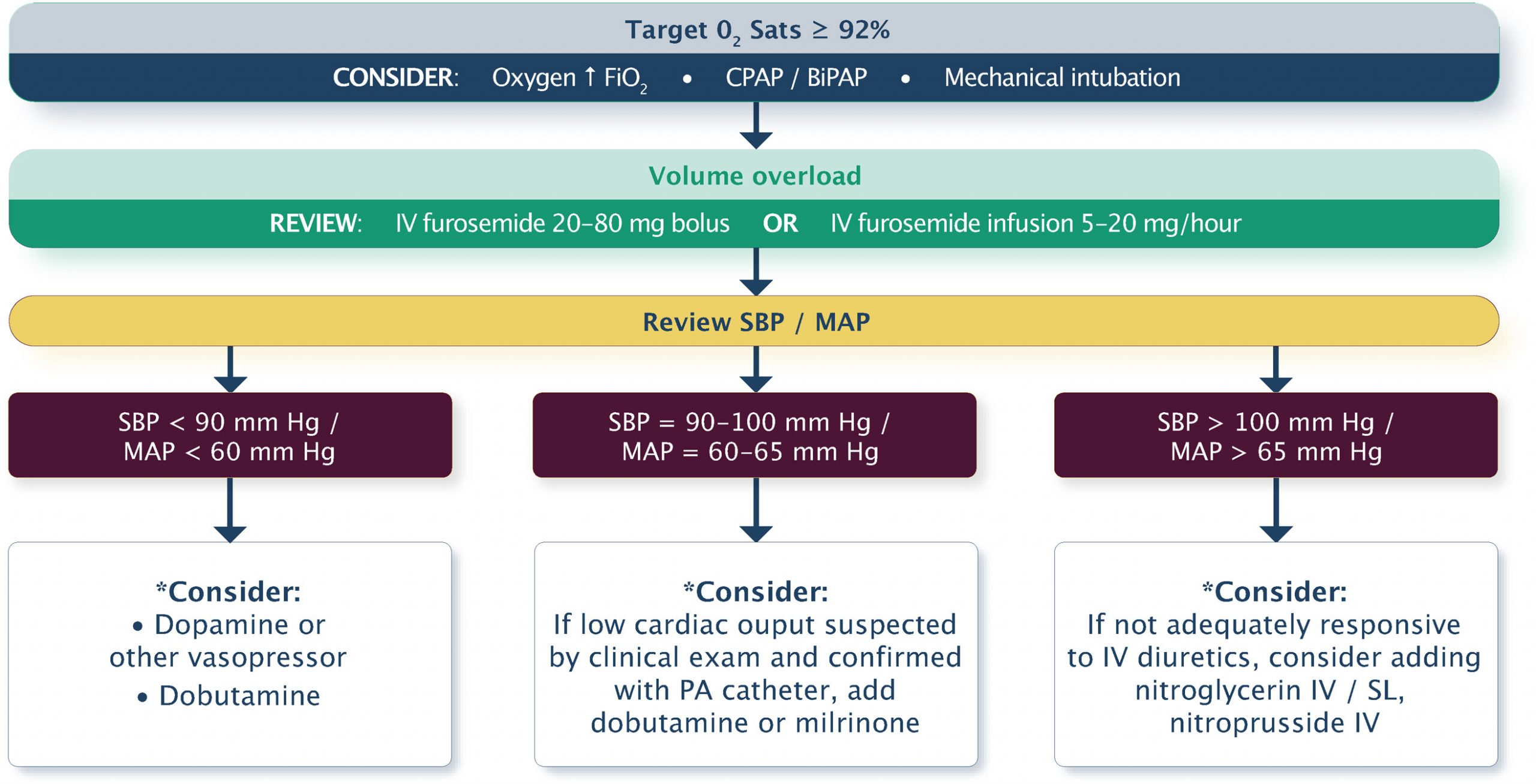
CCS Treatment Algorithm
CCS Treatment algorithm for acute heart failure.
Supportive Care
Supplemental oxygen
Indicated for patients who are hypoxemic, target oxygen saturation above 90%
Potential harm of oxygen on normoxic patients in physiologic studies
CPAP/BIPAP:
Indications:
High respiratory rate (concern for fatigue)
Persistent hypoxemia despite high flow oxygen
Note: Noninvasive ventilation is not recommended for routine use in acute heart failure (3CPO Trial)
Diet:
Cardiac diet with salt (<2g/day) and fluid (<2L/day) restriction
Other:
Urinary catheter should be considered but not needed in clinically stable patients
Central line and/or arterial line should be considered in hemodynamically unstable patients and those that require inotropes/vasopressors
Pulmonary artery catheter should not be routinely used but may be helpful in complex patients used in consultation with Cardiology/Heart Failure Service
Diuretic Therapy
IV Diuretics:
First line therapy for patients with volume overload (pulmonary or peripheral)
IV intermittent dosing recommended over IV continuous as no proven benefit of IV continuous but limits patient mobility
IV high dose (oral dose = IV dose x 2.5, ie. 40 mg PO = 100 mg IV) or low dose (oral dose = IV dose, ie. 40 mg PO = 40 mg IV) are reasonable options with high dose shown to have faster symptom resolution without a significant difference in renal function (DOSE trial)
Diuretic Dosing Guide Adapted from CCS 2017 Heart Failure Guidelines
eGFR
Patient
Initial IV Dose
≥60mL/min/1.73 m2
New onset HF or no current diuretic therapy
Furosemide 20-40 mg 2-3 times daily
Established HF or chronic oral diuretic therapy
Furosemide dose IV equivalent of oral dose
<60mL/min/1.73 m2
New onset HF or no current diuretic therapy
Furosemide 20-80 mg 2-3 times daily
Established HF or chronic oral diuretic therapy
Furosemide dose IV equivalent of oral dose
Other Medical Therapy
IV Vasodilators:
Indication: Relief of dyspnea in hemodynamically stable patients (SBP >100 mmHg)
Options: Nitroglycerin, nesiritide, or nitroprusside; and if not available, nitro patch or oral ISDN can be used
Note: No evidence for reduction of hospitalization or mortality thus should be used for symptom control
IV Inotropes:
Not recommended for routine use for hemodynamically stable patients (i.e. milrinone, dobutamine, dopamine, or levosimendan).
May be used to stabilize patients with low SBP (<90 mmHg), low cardiac output and either euvolemia or hypervolemia (further discussed in pending Cardiogenic Shock topic)
ACE/ARB/ARNI:
Continue if chronic therapy and stable kidney function but do not start new in acute setting (first 8-12 hours)
Beta Blockers:
Continue use unless symptomatic hypotension or bradycardia (consider dose reduction first then discontinuation)
Wait to start new until out of of acute setting and out of heart failure
Monitoring and Discharge
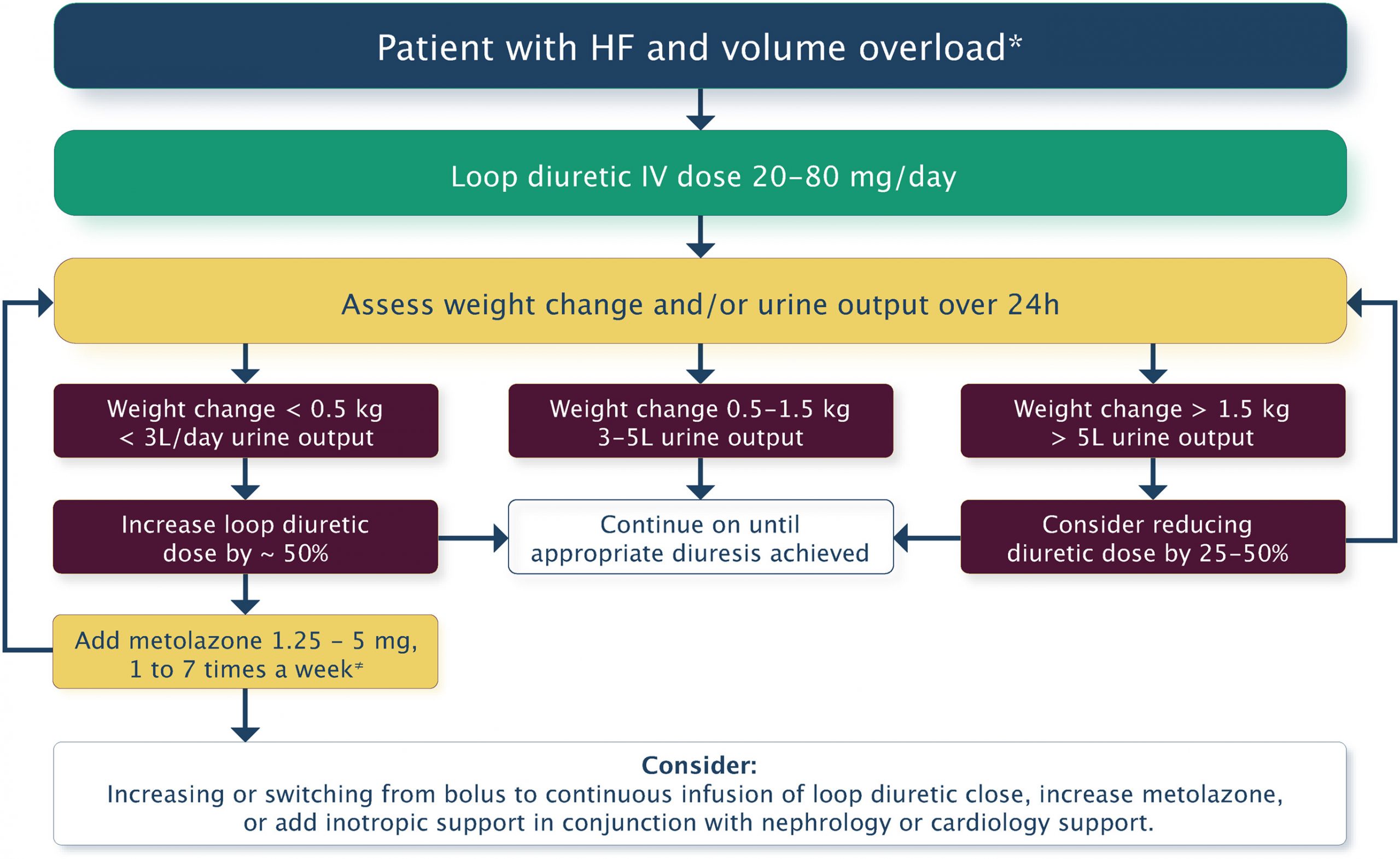
CCS Ongoing Therapy and Monitoring Algorithm
Stepped pharmacologic care
Monitoring and Targets
Monitor patient fluid intake/output and weight
Target net in/ outs of -1L and weight loss of 1kg
If not achieving target, increase diuretic dose by 50%
Practical Tip: If not achieving target at high dose IV lasix (160-240 mg total per day), consider adding metolazone, changing to IV continuous dosing and/or adding inotropic support in conjunction with Nephrology or Cardiology consultation
Discharge
Once euvolemic, transition to lowest dose of oral diuretic to maintain euvolemia
Monitor patient for 24 hours after transition from IV to oral diuretic
Note: Oral furosemide has 50% bioavailability of IV furosemide (Ie. 40mg IV approximates 80mg PO)
Patients should be started on guideline-directed medical therapy before discharge (i.e. Beta blocker, ACE/ARB/ARNI, MRA)
See pending Chronic Heart Failure topic for more information
Readiness for Discharge Adapted from CCS 2017 Heart Failure Guidelines
Symptoms and disease
Stability
Transition
Intercurrent cardiac illness adequately diagnosed and treated
Returned to “dry” weight and stable for > 24 hours
Communication to primary care provider and/or specialist physician and/or multidisciplinary disease management program
Presenting symptoms resolved
Vital signs resolved and stable for > 24 hours, especially blood pressure and heart rate
Clear discharge plan for laboratory tests, follow-up, and other testing
Chronic oral HF therapy initiated, titrated, and optimized (or plan for same)
> 30% decrease in natriuretic peptide level from time of admission and relatively free from congestion
Education initiated, understood by patient, continued education planned