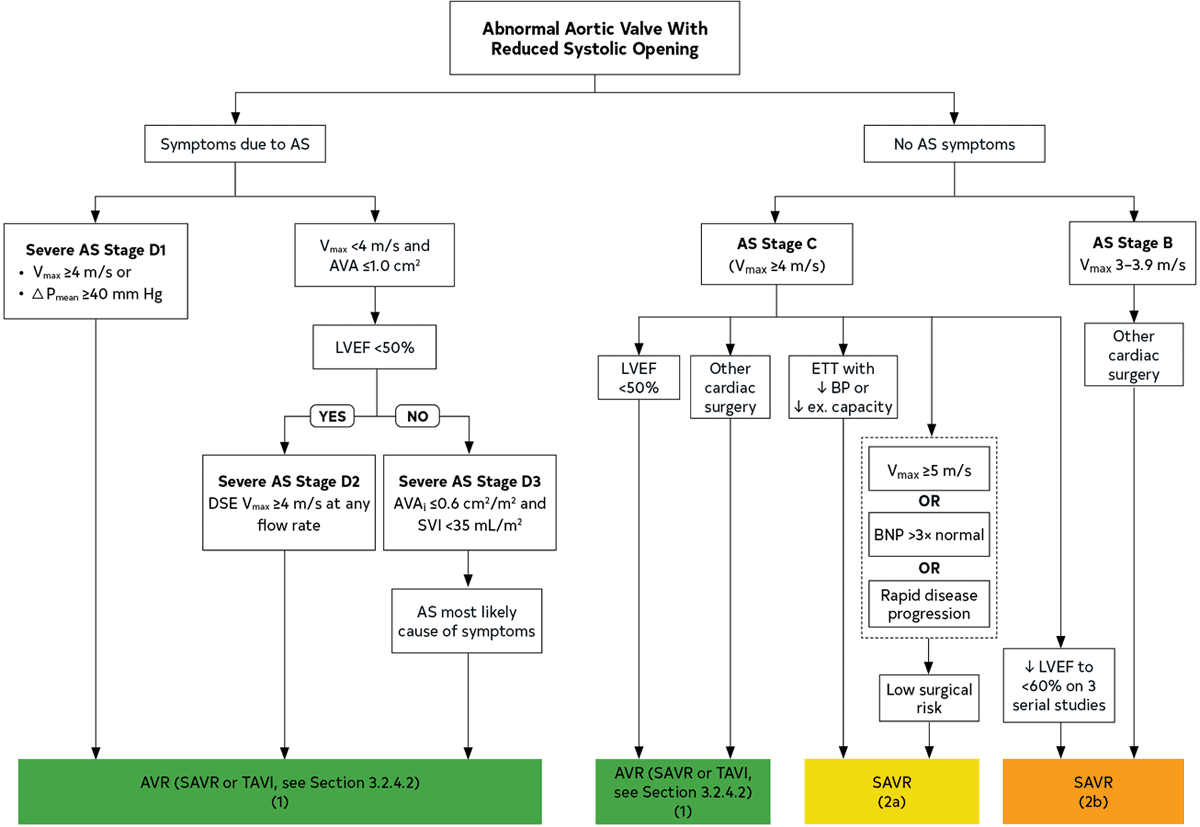
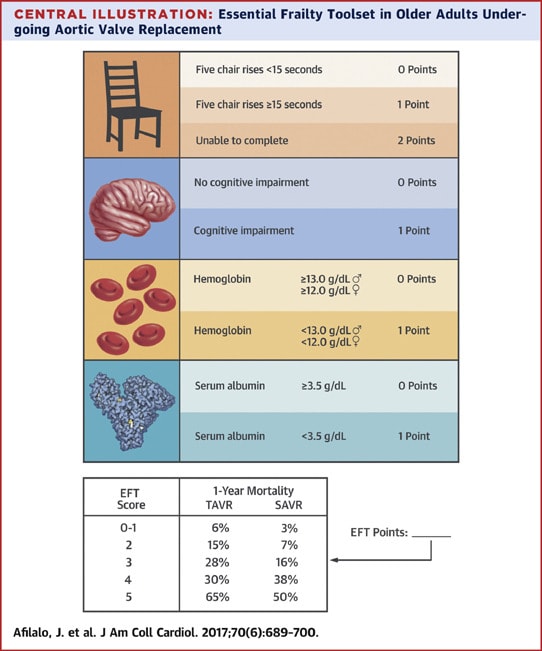
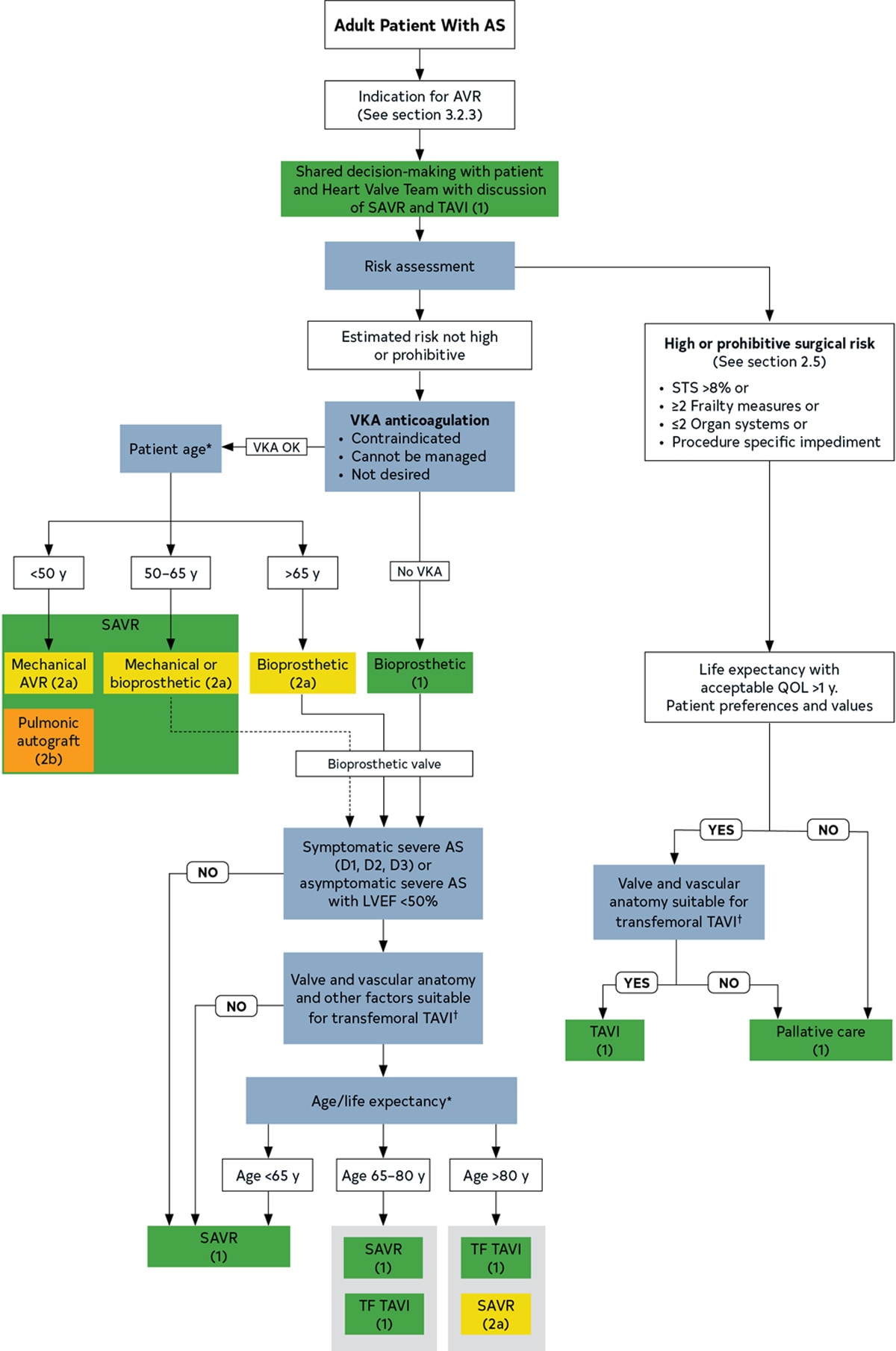
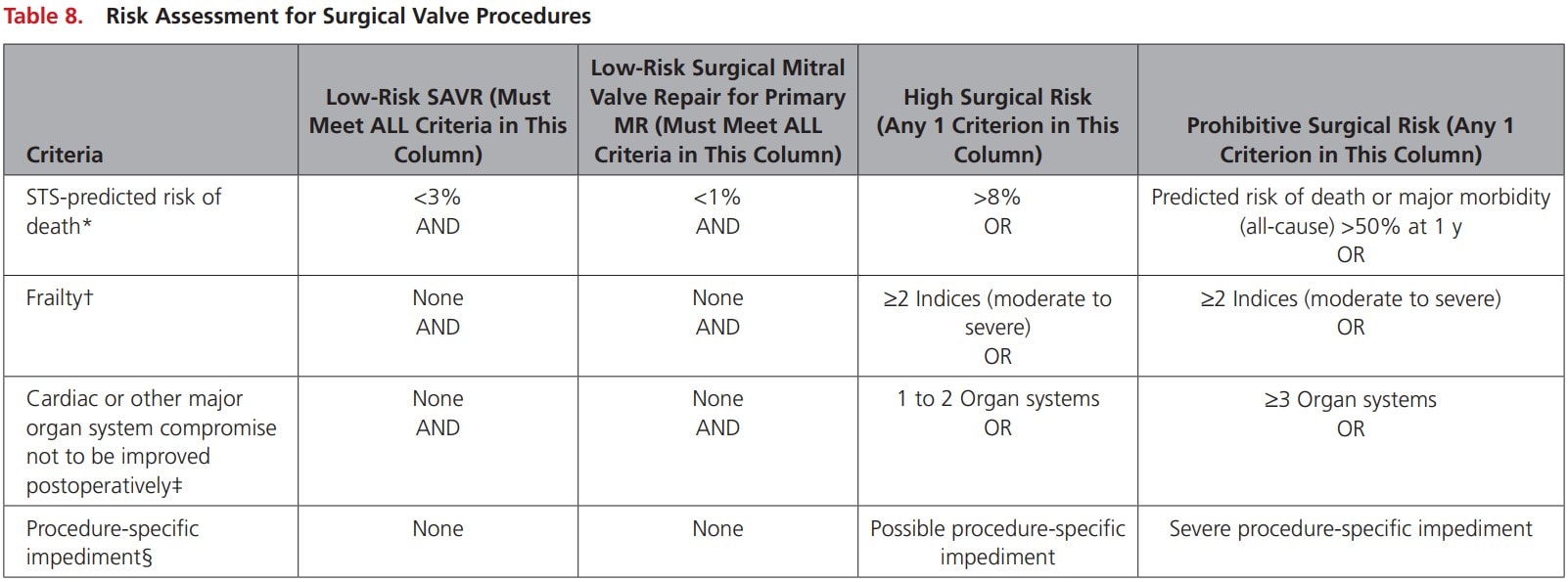
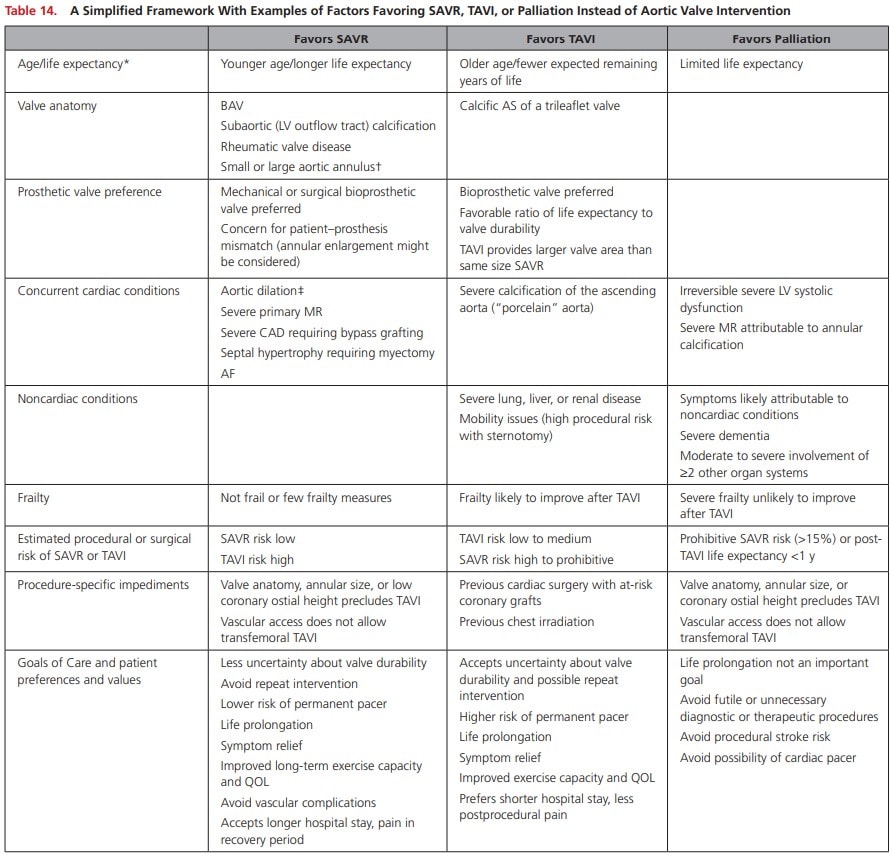
Aortic Stenosis Intervention Abbreviations TTE: Trans-Thoracic EchocardiographyLVEF: Left Ventricular Ejection FractionAS: Aortic Stenosis Introduction Options of fixing stenotic valves include percutaneous vs. open and valvuloplasty vs. replacementDecision should involve a Valve Team and should be individualized to every patientPatient profile and technical factors influence decisionChoosing what type of intervention will be the focus of this article. Diagnosing stenotic lesions and medical therapy are discussed elsewhere. Aortic Stenosis Diagnosis TTE is indicated to establish diagnosisIf low-flow low gradient is suspected, low-dose dobutamine stress testing with echo or cardiac catheterization can be done Criteria Severe aortic stenosis is diagnosed by:Peak velocity >4 m/s or mean gradient >40 mmHgTypically aortic valve area < 1 cm2 but not required to diagnoseAncillary findingsLV diastolic function, LV hypertrophy, and generally normal LVEF, but in late stages EF can drop and LV can dilate Interventions Percutaneous Aortic Balloon DilationSurgical Aortic Valve Replacement (SAVR)Transcatheter Aortic Valve Intervention (TAVI)Ross ProcedureReserved for younger patients AHA 2020 - Timing of intervention for AS Percutaneous Aortic Balloon Dilation Mainly used in young patients; limited role in elderlyCan be used in patients with severe AS and refractory pulmonary edema or cardiogenic shock as a bridge but less common with availability of TAVI Prosthetic Valve Choice Choice of AVR should be based on shared decision making involving the Valve Team and the patient Assess Risk and Frailty Use either STS score or EUROSCORE II to assess risk (note – maybe we could include images of these scores as quick references too? Just a thought)Use ADLs or frailty scores such as the FRAILTY-AVR 4 point score to assess frailty Afilalo 2017 - FRAILTY-AVR 4 point score High or prohibitive risk patients should go for TAVI or palliationNot high risk:<50 SAVR (mechanical valve)unless contraindication to VKA50-65 SAVRMechanical or bioprosthetic valveHighly debated as new bioprosthetic valve more durable65-80 SAVR or TAVI>80 TAVI (Class 2 SAVR) AHA 2020 - Choice of SAVR versus TAVI when AVR is indicated for valvular AS Assess TAVI Suitability TAVI suitability should be assessed by Valve TeamAssessment includes valve anatomy, annular size, coronary ostial height (low ostial height precludes TAVI) and vascular access Decision Making Frameworks AHA 2020 - Risk Assessment for Surgical Valve Procedures AHA 2020 - A Simplified Framework With Examples of Factors Favoring SAVR, TAVI, or Palliation Instead of Aortic Valve Intervention Further Reading 2020 AHA: Guideline for the Management of Patients With Valvular Heart Disease (html) (pdf)Afilalo J, Lauck S, Kim DH, et al. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J Am Coll Cardiol. 2017; 70(6):689-700. (html) Authors Author: Atul Jaidka (MD, FRCPC, Cardiology Fellow)Copy Editor: Megha Shetty (MD Candidate)Last Updated: April 5, 2021Comments or questions please email feedback@cardioguide.ca Post author:Atul Jaidka Post published:April 6, 2021 Post category:Cardio Topics / Valvular Heart Disease