Acronyms
HR – Heart Rate
SA – Sinoatrial
AV – Atrioventricular
RA – Right Atrium
SVC – Superior Vena Cava
LAD – Left Anterior Descending
R/L BBB – Right / Left Bundle Branch Block
Introduction
- For management, see “Management of Bradycardia”
- Bradyarrhythmia is defined as a HR<60bpm.
- The etiology of bradyarrhythmia is numerous and can be associated with physiological or pathological states.
- The level of disturbance in the cardiac conduction system responsible for the bradyarrhythmia is an important marker of prognosis and dictates the management strategy.
- Understanding indications for pacemaker implantation is key.
Clinical Features
- Clinical presentation varies in severity depending on the degree of cardiac output.
- Can be asymptomatic, and only incidentally discovered on the ECG.
- Common symptoms:
- **Cardiac syncope** – most important symptom.
- Cardiac syncope generally presents as a sudden unexpected loss of consciousness without any prodrome or postdrome.
- Represents periods of ventricular asystole.
- Mild bradycardia symptoms can be present, but are non-specific. Patients can report fatigue, exercise intolerance, dyspnea, anginal pain, pre-syncope
- **Cardiac syncope** – most important symptom.
Anatomy of the Conduction System
- Impulses generated through the automaticity of the SA node propagate through the atria and reach the AV node.
- The AV node then conducts incoming impulses to the His bundles, and the Purkinje fibres, which distribute the signals throughout the myocardium.
- Sinus activation originates from sinoatrial node (automaticity).
- Located at the junction of the SVC and RA (crista terminalis).
- Blood supply to the SA node is from the sinoatrial node artery.
- The sinoatrial node artery arises from right coronary artery (55%), left circumflex (35%) or is dual supplied by both (10%).
- Serves as the electrical connection between atria and ventricles and modulates incoming impulses from the SA node.
- Can serve as a subsidiary pacemaker.
- Blood supply to the AV node is from the AV nodal artery.
- AV nodal artery arises from posterior descending artery (80%), left circumflex (10%) or dual supplied by both (10%).
- Also receives collateral blood supply from left anterior descending artery (relatively less susceptible to ischemia).
- Conduct impulse to the ventricular myocardium.
- The left bundle branch gives rise to anterior fascicle and posterior fascicle.
- Relatively less influenced by the autonomic nervous system compared to SA and AV node.
- Blood supply from both the AV nodal artery and septal perforators of left anterior descending (LAD).
- Anterior fascicle = blood supply only from septal perforators of LAD.
- Posterior fascicle = blood supply from both septal perforators of LAD and posterior descending artery.
Etiology
- Etiologies are divided into intrinsic (pathophysiological processes inherent to the conduction system) or extrinsic (external processes influences the function of an intact conduction system).
- Another way to separate the differential diagnosis is by the following categories:
- Irreversible – Acquired Pathologic
- Idiopathic/degenerative ** MOST COMMON **
- Systemic Illness (Sarcoid, Lyme, Endocarditis)
- Reversible
- Neurogenic (i.e. vasovagal)
- Metabolic
- Drugs (i.e. beta-blockers)
- Irreversible – Acquired Pathologic
- Idiopathic degenerative fibrosis (aka Lenegre disease)
***MOST COMMON*** - Infection/Inflammatory
- Infective Endocarditis
- Lyme Disease
- Sarcoidosis / Myocarditis
- Others: Chagas disease, Diphtheria, Tuberculosis, Measles, Mumps, Toxoplasmosis, Sarcoidosis
- Infiltrative disease
- Amyloidosis, Hemochromatosis, Lymphoma
- Ischemia/Infarction
- Collagen vascular disease
- Rheumatoid arthritis, Scleroderma, SLE, Polymyositis
- Surgical or procedural trauma
- Cardiac ablation or catheterization, Congenital heart disease repair, Valve replacement, Myomectomies, Radiation
- Neuromyopathic disorders
*Table is reproduced in part from the 2018 ACC/AHA/HRS Guidelines on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay.
- Autonomic perturbation:
- Carotid sinus hypersensitivity
- Vasovagal syncope
- Situational syncope (cough, defecation, glottic stimulation, micturition, vomiting)
- Excessive vagal tone
- Conditioned athletes (normal)
- Sleep
- Metabolic
- Hyper/hypokalemia, Acidosis, Hypothermia, Hypothyroidism, Addison’s disease
- Drugs
- Beta-blockers, CCB, digoxin, antiarrhythmic drugs, sympatholytic agents (e.g., clonidine), lithium, amitriptyline, phenytoin, prednisone
- Increased intracranial pressure
- Sepsis
*Table is reproduced in part from the 2018 ACC/AHA/HRS Guidelines on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay.
Sinus Node Dysfunction
- Sinus bradycardia: Sinus rate <50 bpm, with P-waves upright in leads I, II and aVL and negative in aVR
- Sinus pause: >3 seconds between consecutive sinus node depolarizations.
- Sinus arrest: Complete failure of impulse formation in the SA node. Absence of atrial depolarization on ECG (no sinus P-waves)
- Sinoatrial exit block: Failure of normal sinus impulse to conduct to the atria due to delay in conduction within or around the SA node.
- Chronotropic incompetence: Inadequate ↑ in HR in response to increased demand.
- Resting ECG will be normal. Exercise testing will reveal blunted HR response (failure to achieve HR 100-120bpm at max. effort, or plateau at <70-80% of max HR at peak effort)
- NOTE: An inpatient with suspected chronotropic incompetence can be simply ambulated with a monitor to ensure heart rate accelerates with activity.
- Tachycardia-bradycardia syndrome: Alternating periods of bradyarrhythmia with tachyarrhythmia
- Classically this syndrome refers to atrial fibrillation with conversion pauses, which happens when the sinus node does not recover after periods of AF.
- The term “tachy-brady syndrome” is vague and colloquial.
- Learners are urged to be more specific about the diagnosis (for example “atrial fibrillation with conversion pauses”), rather than using the term “tachy-brady” as a blanket statement for anyone with tachycardia and bradycardia.
- Sinus arrhythmias: The SA node fires at a regular rate. Sinus arrhythmia refers to the irregularity in sinus rate or pauses.
- NOTE: None of the above diagnoses are strict indications for pacing. However, if the patient is symptomatic, pacing can be considered to improve symptoms.
Atrioventricular Conduction System Abnormalities:
First degree AV block
- PR interval >200 msec, all P-waves produce a QRS.
- Normal AV nodes can have a slow pathway. When it conducts, a long PR interval is observed.
- Term term 1st degree AV block is a misnomer because it represents a conduction delay rather than a block.
- 1st degree AV block can be physiologic.
- Rarely has clinical importance.
Second degree AV block
- Some P-waves are not followed by QRS complexes (aka “blocked”)
- There are two ways to classify second degree AV block:
- Mobitz I (wenckebach) vs Mobitz II
OR - AV nodal vs infra-His block
- Mobitz I (wenckebach) vs Mobitz II
- NOTE: Mobitz I or II is an observation of a pattern on ECG, whereas AV node vs infra-His is a diagnosis with specific management.
- AV Nodal block is usually physiologic. The function of the AV node is to block atrial stimuli from activating the ventricles too quickly. The AV node can block additional impulses in response to autonomic input.
- For example: many healthy young patients can have AV nodal block during sleep when vagal tone is high – leading to the Wenckebach phenomenon on the monitor. Patients with AV nodal block have a good prognosis, and do not require pacemakers unless symptomatic.
- Infra-His block is a block of conduction fibers that connect the AV node to the ventricles. These fibres should not regularly block signals, and an infra-hisian block is usually pathologic, has a poor prognosis, and requires a pacemaker in most cases whether or not the patient has symptoms.
- AV Nodal block is usually physiologic. The function of the AV node is to block atrial stimuli from activating the ventricles too quickly. The AV node can block additional impulses in response to autonomic input.
Mobitz Type I
- Progressive prolongation in the PR interval before blocked P-wave.
- Hint is a group beating pattern on ECG
- For advanced learners: Typical features of Wenckebach:
- Progressive prolongation of PR interval in Wenckebach cycle.
- R-R interval progressively shortens as a result of the decreasing increment in PR interval prolongation over the Wenckebach cycle.
- PR interval after the block tends to be shorter than the one preceding the block.
- Duration of the pause is less than twice the R-R interval of the preceding conducted beats.
- Wenckebach phenomenon indicates a block in decremental tissue, which is a property of the AV node. Hence, Mobitz I/Wenckebach pattern suggests a block in the AV node. (Rare cases are published of infra-His wenckebach)
- For advanced learners: Typical features of Wenckebach:
Mobitz type II
- PR interval remains constant prior to blocked P-wave.
- The PR interval can be normal or prolonged.
- Almost always represents infra-Hisian block, which is pathologic. Infra-His fibers do not usually have decremental properties.
2:1 AV block
- Every second atrial impulse fails to conduct to the ventricle.
- Cannot be classified into Mobitz I or II readily (cannot discern a PR pattern from only one preceding conducted beat).
- “2:1 AV block” is separate from Mobitz I and Mobitz II. Just like mobitz I and II, it is an ECG observation not a diagnosis.
- The clinician must identify if AV block is AV nodal (good prognosis) or infra-Hisian (poor prognosis)
- Certain features can suggest location of block:
| Feature | AV Nodal | Infra-Hisian |
|---|---|---|
| Presence of conduction system disease (RBBB/LBBB/etc..) | Absent (Narrow QRS) | Present (Conduction Abnormalities) |
| PR Interval | Long PR (> 300ms) | Normal PR |
| Atropine (increases sinus rate – which is the rate of input into AV conduction system) | Improves the block | Worsens the block by increasing the activation rate of diseased conduction tissue (can cause high-grade block) |
| Response to exercise (adrenergic stimulus) | Improves | Worsens |
The most important investigation in a patient with 2:1 AV block is additional ECGs and/or rhythm monitoring (telemetry or Holter). If the block is AV nodal, eventually you may see wenckebach phenomenon or an improvement with activity. If the block is infra-His, you may see higher grade block.
High-grade AV block
- Two or more consecutive P-waves fail to conduct.
- This is an observation, and does not suggest the level of the block. Usually high-grade AV block is infra-Hisian, but can be AV-nodal with significant vagal tone (i.e. vasovagal episode).
Third degree AV block
No atrial impulses are conducted to the ventricle (AV dissociation).
| Criteria for Complete AV block (3rd degree) |
|
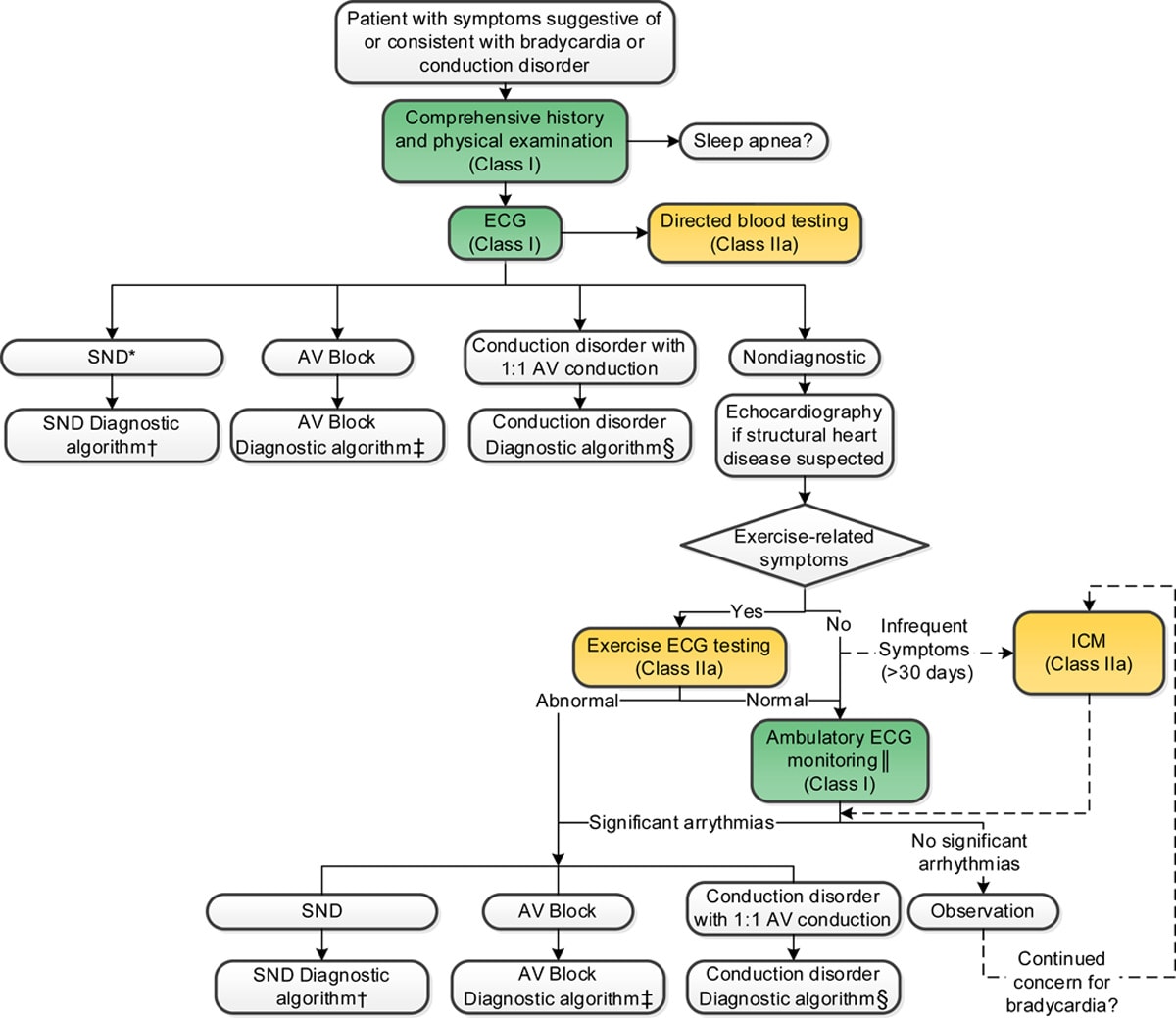
Approach to Evaluation
Step 1: Patients with suspected bradyarrhythmia or conduction disorder should have a comprehensive history and physical examination (Class I) and ECG (Class I) completed. Blood work may be indicated depending on the suspected etiology (Class IIa)
History:
- Determine the timing, severity, duration, and frequency of symptoms.
- Ask about triggers and alleviating factors.
- Establishing the relationship between the symptoms and the associated triggers can help narrow the differential.
- Potential associated factors: positional change, prolonged standing, emotional or physical stress, medication, food, micturition, defection, and tight collars.
- Past history of cardiac disease or cardiovascular risk factors may suggest intrinsic pathology of the conduction system.
- Thorough review of medications (both prescription and over the counter)
Physical Exam:
- Orthostatic vitals can help determine the presence of autonomic dysfunction and suggest a diagnosis.
- Look for evidence of adequate perfusion (mental status, capillary refill and temperature at extremities, urine output etc.)
- Look for evidence of underlying heart disease or systemic disease (See Etiology Table).
- Carotid sinus massage if suspecting carotid hypersensitivity syndrome (if not contraindicated, i.e. no ipsilateral carotid bruit).
- NOTE: Bradycardic patients can be normo-tensive but still be in shock due to reduced cardiac output. Urine output and mental status can be clues to reduced cardiac output.
ECG: See ECG features
- If exercise related symptoms, consider exercise ECG.
- Patients can be ambulated in clinic/ED to determine if their heart rate accelerates. This can help identify chronotropic incompetence (alternatively a Holter monitor can help identify heart rate variability throughout the day).
- If symptoms are infrequent, consider extended cardiac rhythm monitoring (See non-invasive testing)
Diagnostic Testing
Non-invasive:
- ECG: Monitoring period depends on the frequency of the symptoms and suspected arrhythmia.
Device | Description | Recording duration |
Holter monitor | External device with leads worn constantly, that continuously records ECG. | 24-72 hours |
Event monitor | External device the stores recorded ECG only when triggered by patient (i.e., during awake symptomatic event). | Weeks |
External loop recorder | External device, that is worn constantly for the recording period. Can be patient-activated or auto-triggered. Has memory loop capabilities (will store recording immediately preceding and after the triggered event). | Weeks |
Implantable loop recorder | Subcutaneously implanted device. Operates similar to the external loop recorder. – Best choice for infrequent symptoms (>30d between episodes) | Up to 3 years |
Further Reading
Authors
- Authors: Drs. Yehia Fanous (MD, FRCPC, Internal Medicine Resident), Atul Jaidka (MD, FRCPC, Cardiology Fellow), Dr. Pavel Antiperovitch (MD, FRCPC, EP Fellow)
- Staff Reviewer: Pending (MD, FRCPC[Cardiology])
- Copy Editor: Donald Bastian (MD Candidate)
- Last Updated: February 25, 2021
- Comments or questions please email feedback@cardioguide.ca