Life threatening acute complications of MI includes the following differential:
Mechanical Complications:
LV free wall rupture –> Leads to cardiac tamponade
Ventricular septal defect –> Leads to RV volume overload and shock
Papillary muscle rupture –> Leads to acute severe mitral regurgitation, causing pulmonary edema and shock.
LV pseudoaneurysm (aka “contained rupture”) – myocardial rupture, but saved by pericardial adhesions.
Non-Mechanical Complications
AV block –> Usually intermittent due to vagal etiology, but sometimes due to direct ischemia/infarction, which is permanent.
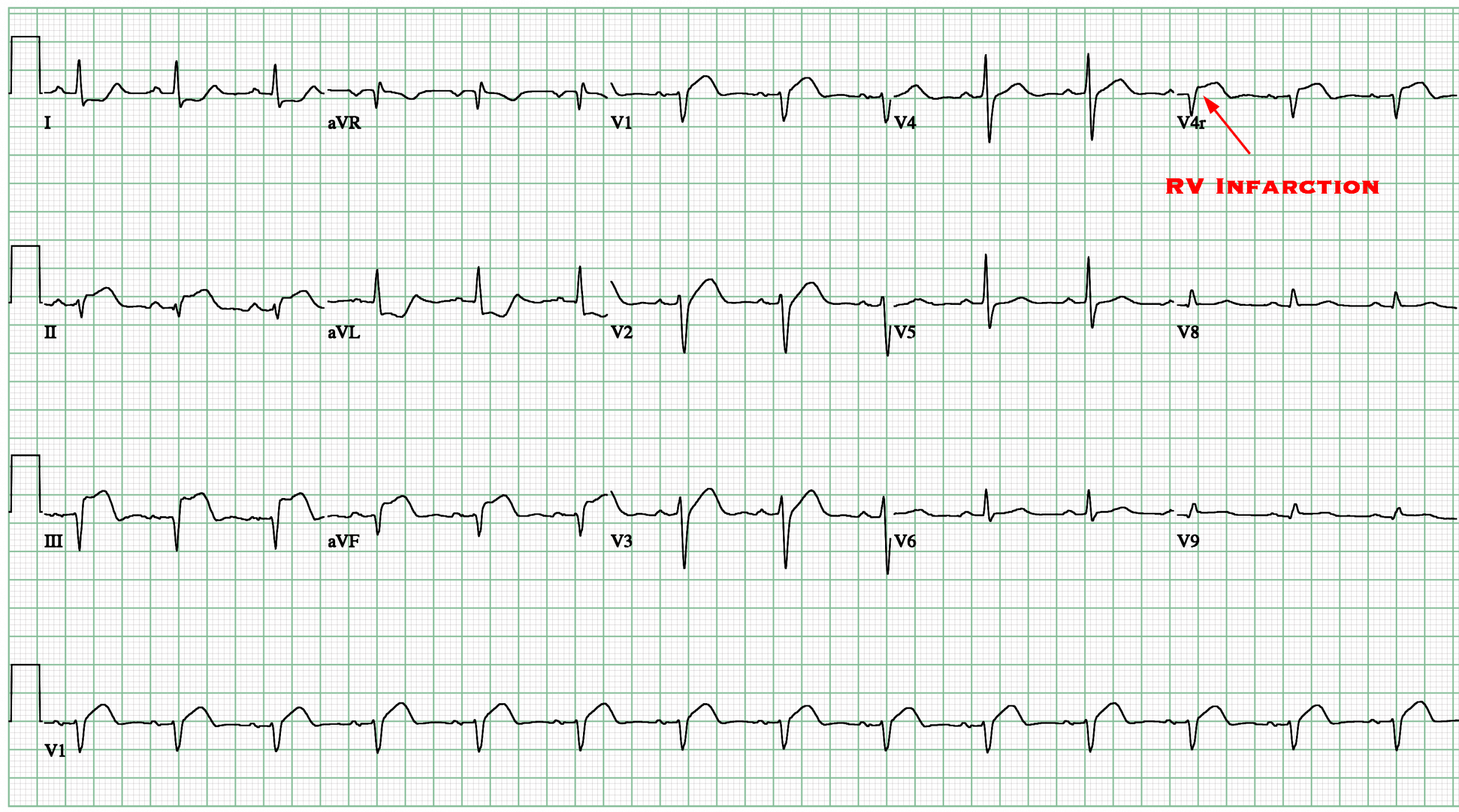
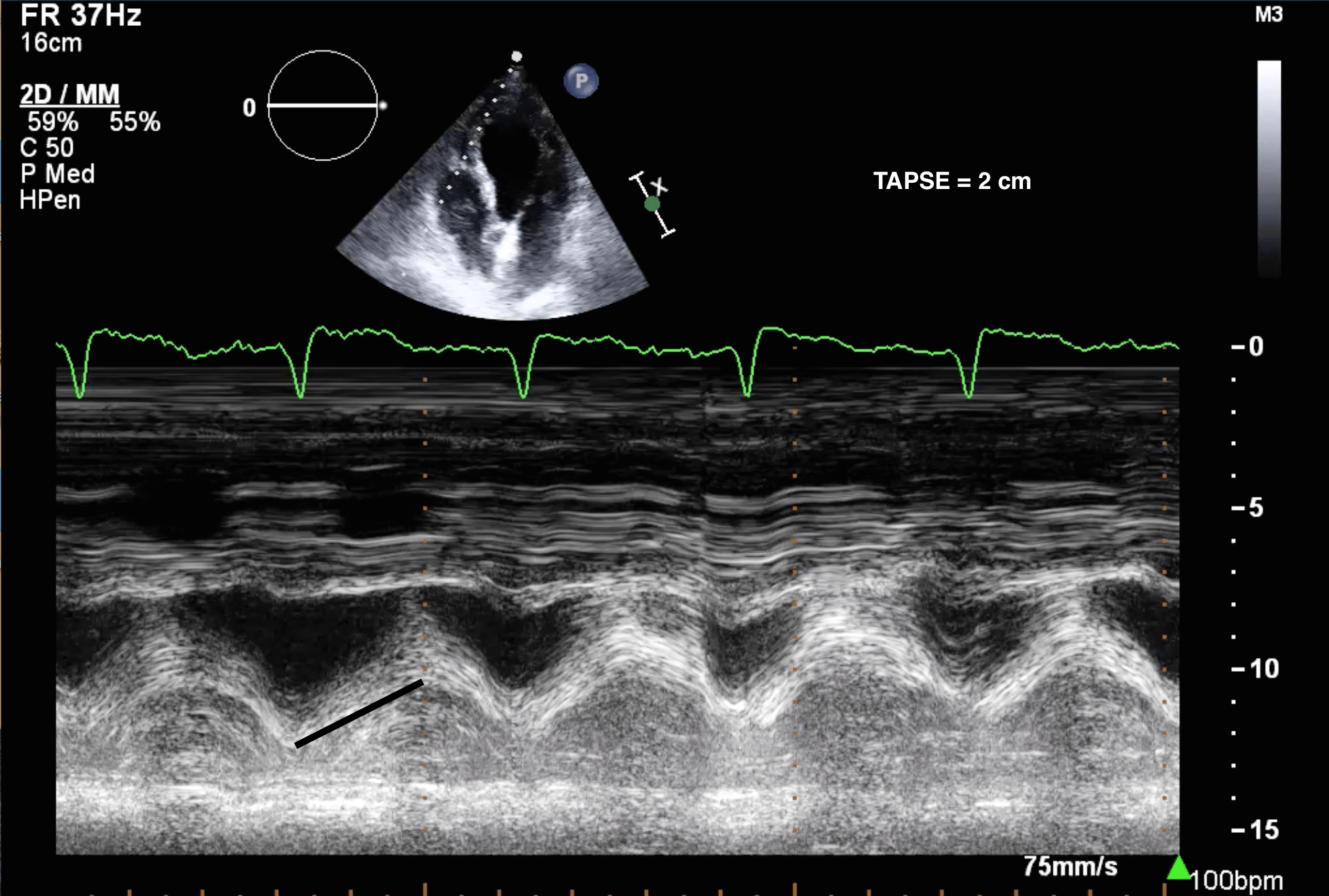
RV Infarct –> Severe RV failure, classically presenting with hypotension/shock, RV volume overload and no pulmonary edema.
LV thrombus –> Very high risk of stroke.
A mechanical complication of MI must be suspected if:
The patient presents in shock or acute pulmonary edema
A prominent murmur is auscultated
Late presentation MI after resolution of ischemia
If a mechanical complication is suspected:
Urgent structural assessment is required with a bedside echocardiogram/POC-US.
The benefit of a second antiplatelet agent must be reassessed. ASA is usually acceptable, however if a mechanical complication is highly suspected, a second antiplatelet agent may need to be withheld until further assessment with urgent cardiac imaging. If surgery is required, second antiplatelet agent should be avoided, if possible, to reduce the risk of operative bleeding.
Clinicians may choose a short-acting anticoagulant, such as heparin, which can be easily reversed if urgent surgery is needed.
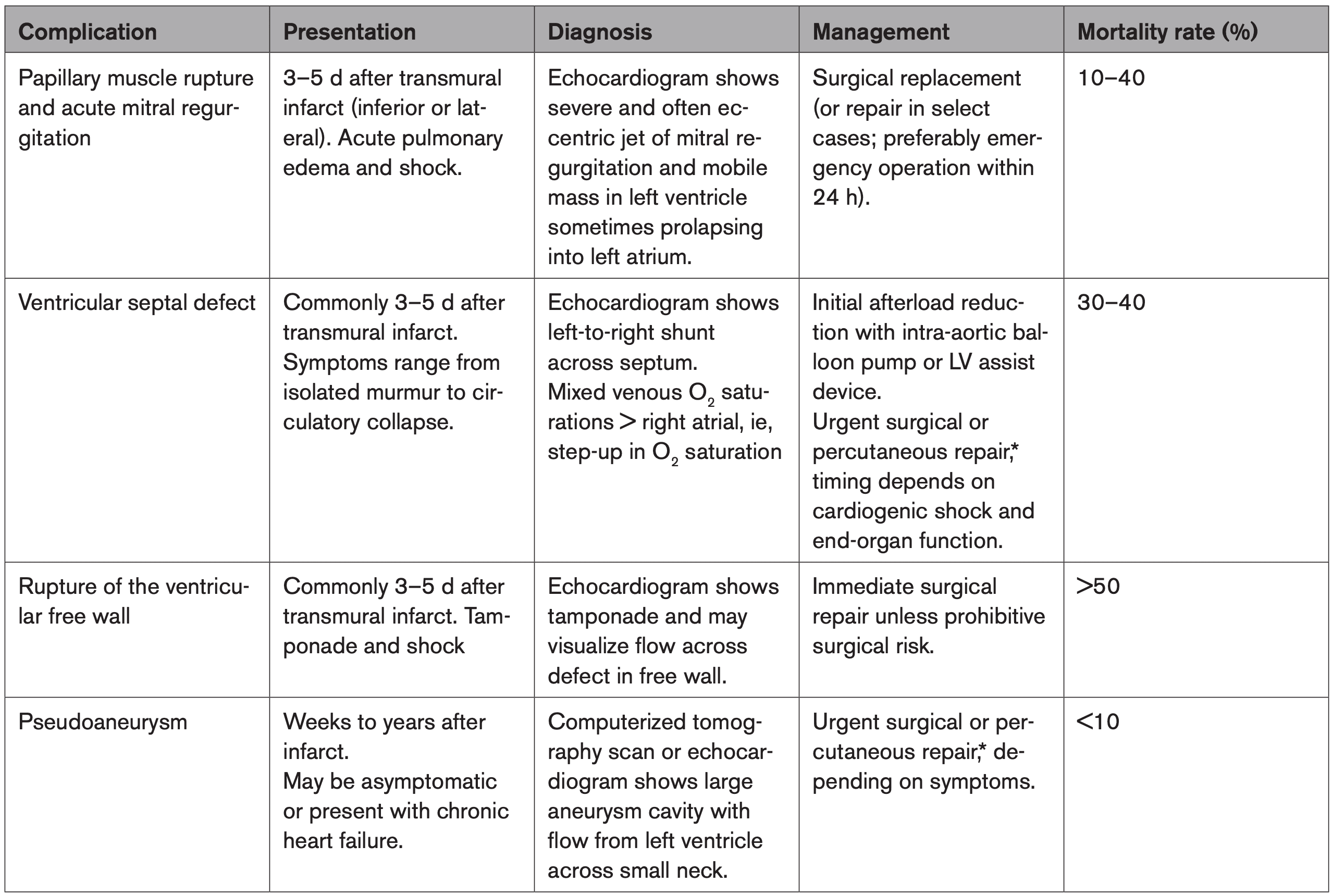
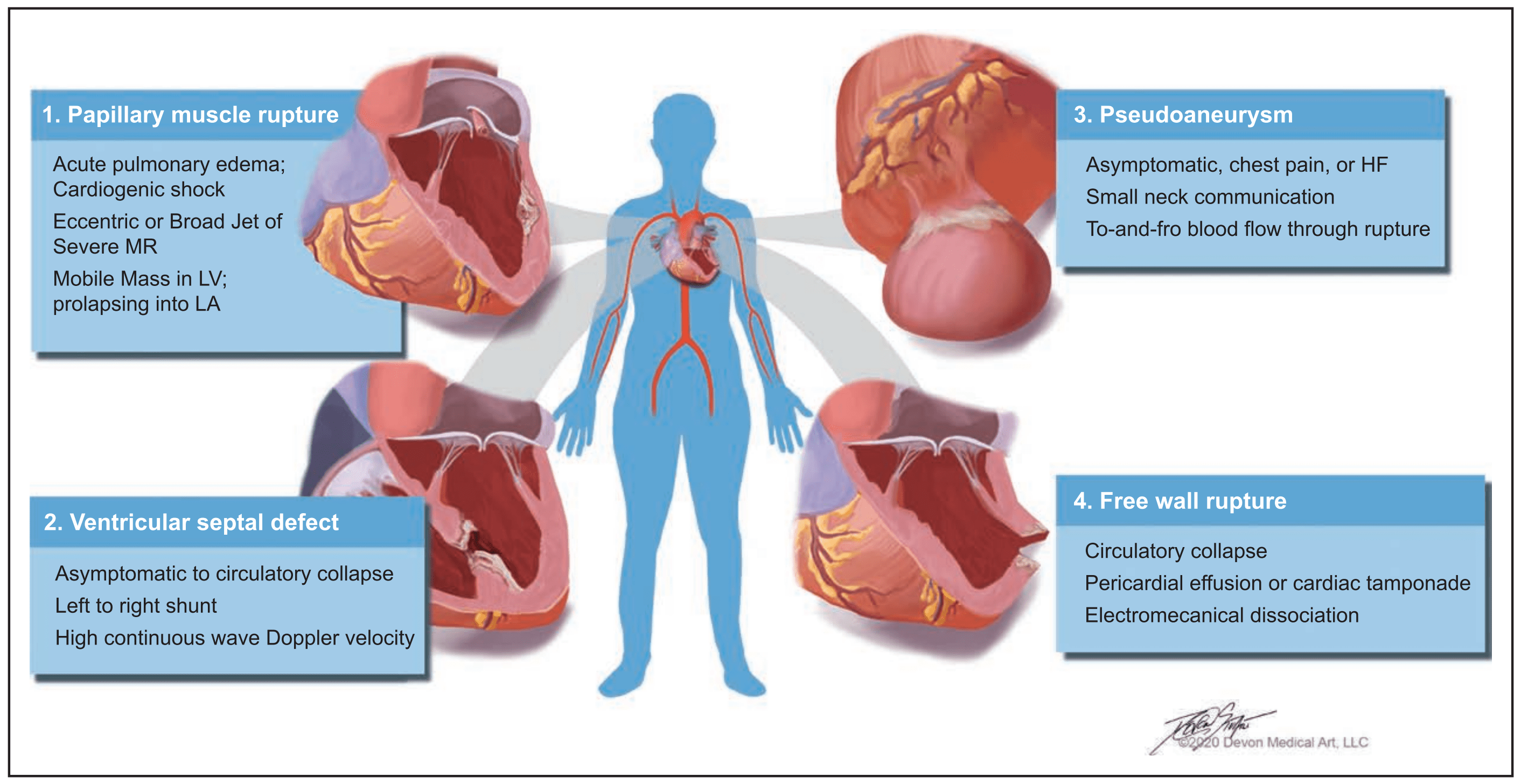
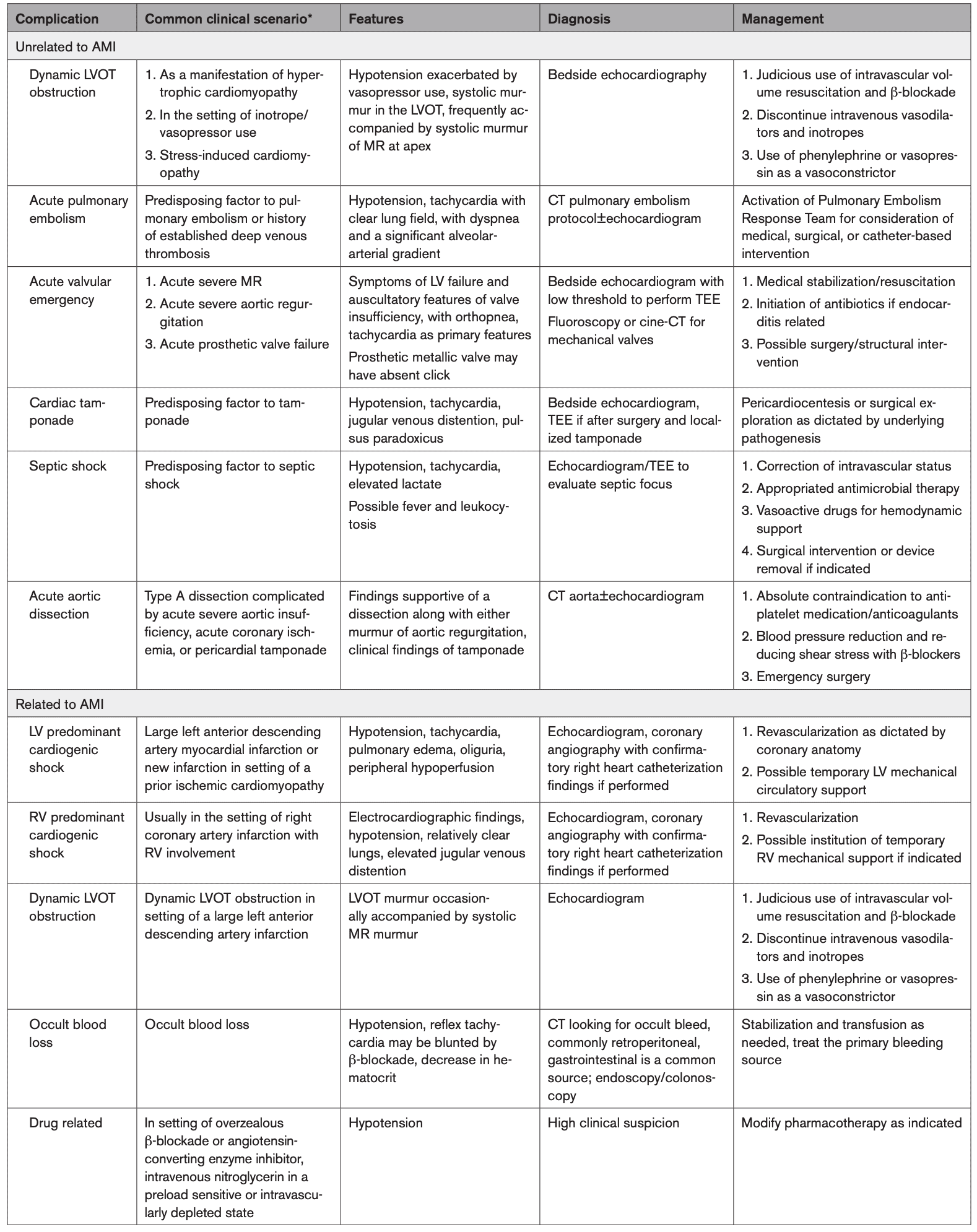
AHA 2021: Summary of Major Mechanical Complications of Acute Myocardial Infarction
AHA 2021: Clinical characteristics of mechanical complications of acute myocardial infarction
Left Ventricular (LV) Thrombus
LV thrombus is usually seen in patients presenting with large anterior STEMIs
Late presentation is an important risk factor
LV thrombus results from the “perfect storm” of factors contributing to “Virchow’s Triad:”
LV wall akinesis/dyskinesia resulting in stagnant blood flow
Pro-coagulative state
Ischemia resulting in inflammation
The incidence of LV thrombus is about 5-7% in anterior MI.
(Number may be smaller with modern reperfusion times)
Imaging options:
Echo (most commonly used)
CT or MRI.
LV thrombus forms 12-72 hours after MI.
Imaging too early in the MI course may not identify an LV thrombus
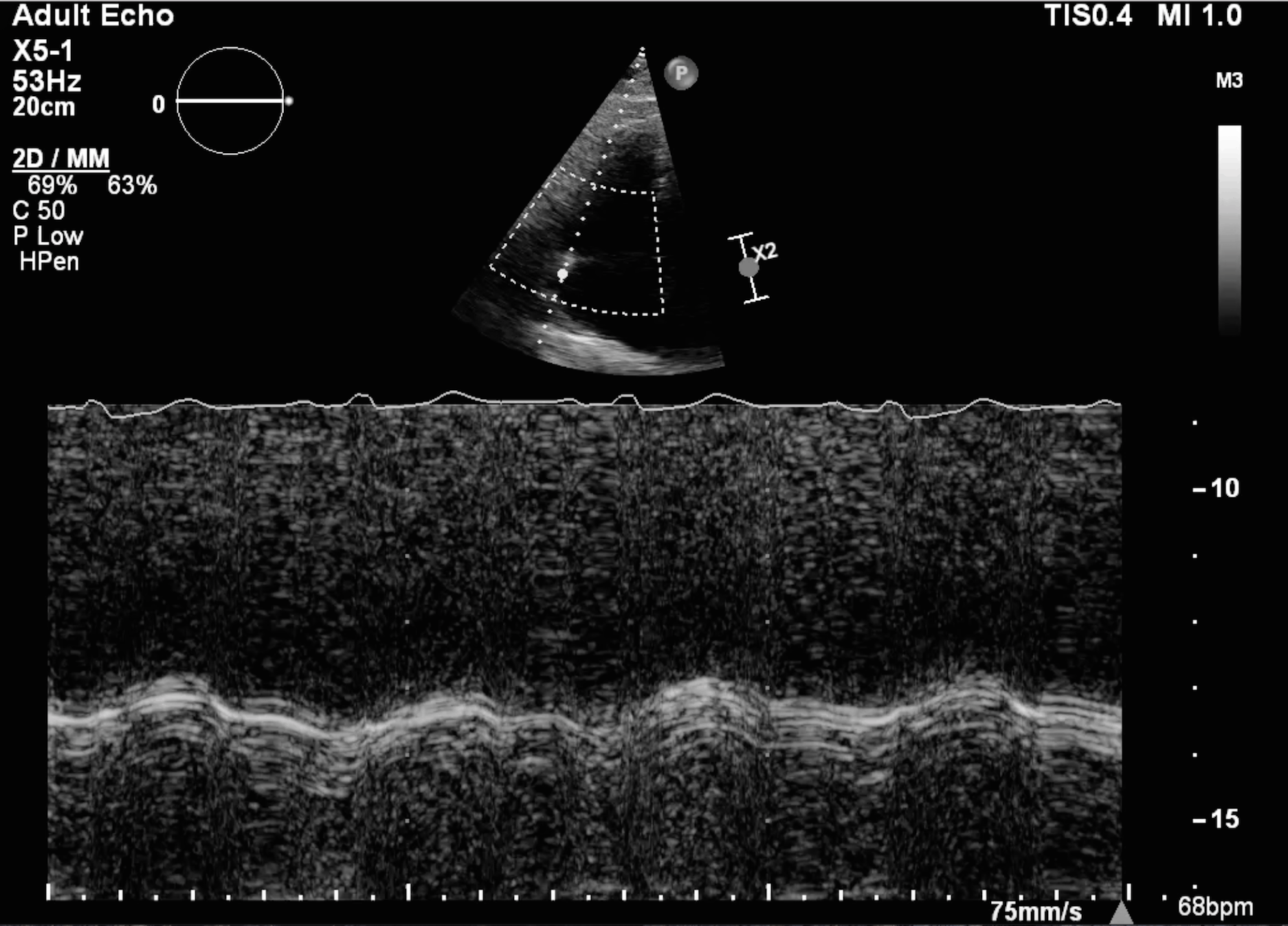
Parasternal long axis view. This patient has antero-septal and apical akinesis likely due to an anterior MI.
Apical 4 chamber view showing an apical wall motion abnormality. There is apical drop-out, which makes diagnosis of LV thrombus difficult. Echo contrast is required.
Contrast enhanced scan demonstrating a filling defect at apex consistent with an LV thrombus.
Zoomed apical view with contrast showing a filling defect consistent with an LV thrombus.
Parasternal Long Axis
Apical 4 Chamber
Contrast
Contrast Zoom
Treatment of LV Thrombus
The most dreaded complication of LV thrombus is stroke.
Treatment of LV thrombus
Vitamin K antagonists (VKAs)
DOACs are available, but only used if VKA-intolerant (no clinical trials available, case reports only)
Prevention of LV thrombus in anterior MI
CCS 2018 – No routine anticoagulation (citing poor evidence and high risk of bleeding)
AHA 2013 – Class IIB indication for anticoagulation
Generally treat with anticoagulation for 3-6 months, and repeat echo to reassess whether the LV thrombus has resolved.
Chronic LV thrombus (> 3-6mo) often becomes “mural”, and has a significantly lower embolic risk. Many clinicians switch to a DOAC at that point to reduce the risk of bleeding, however no clinical practice guidelines or clinical evidence helps guide the management of chronic LV thrombus (as of Jan 2021).
CCS 2018 Heart Failure Guidelines
We recommend against routine anticoagulation after large anterior MI and low EF, in the absence of intracardiac thrombus or other indications for anticoagulation (Weak Recommendation; Low-Quality Evidence).
AHA 2013 STEMI Guidelines
Anticoagulant therapy may be considered for patients with STEMI and anterior apical akinesis or dyskinesis. (Class IIB) (Level of Evidence: C) (Duration: 3 months. INR 2.0-2.5 if used with DAPT)
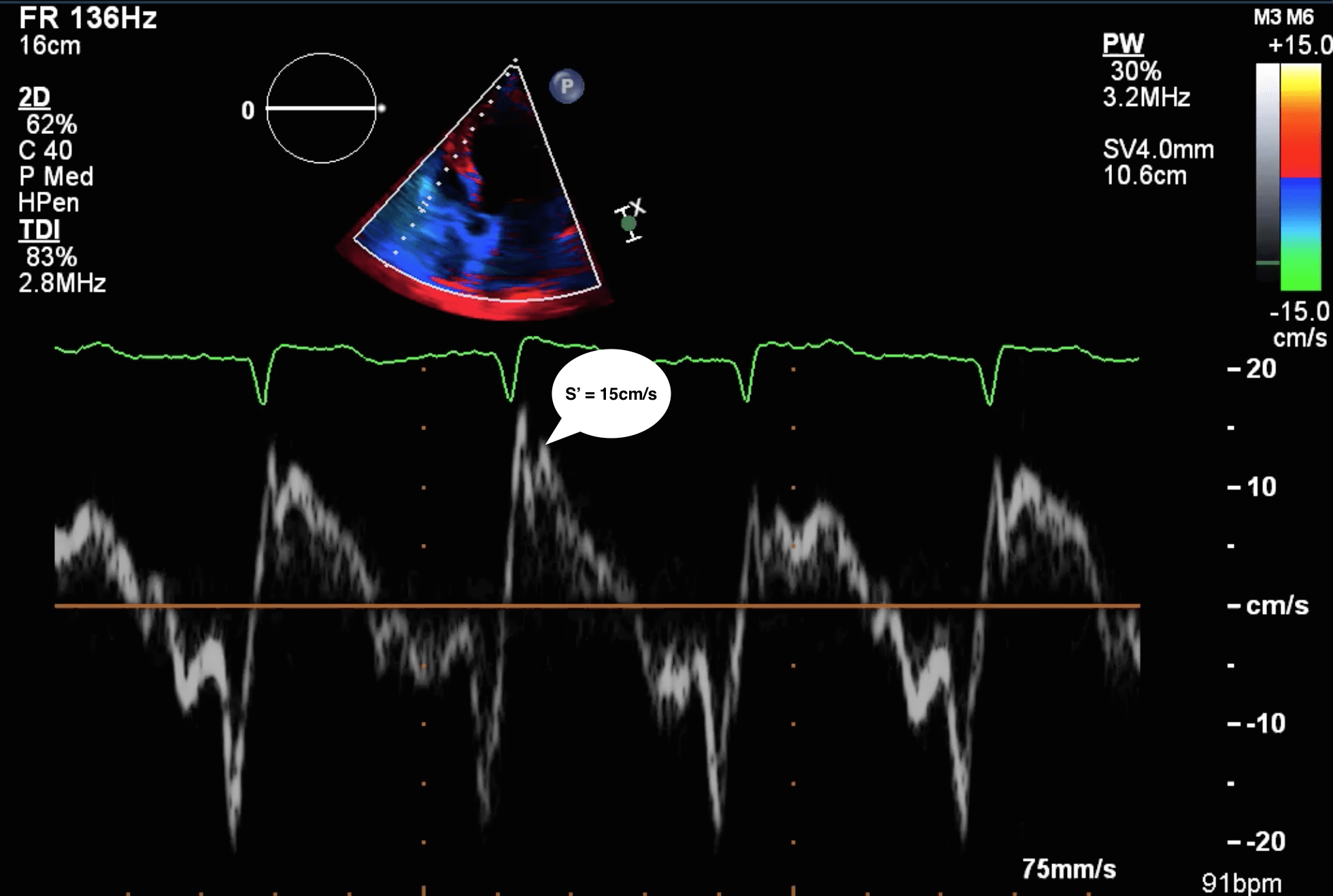
Even after revascularization, the right ventricle may take some time to recover.
Hypotension Management
The main hemodynamic problem resulting from an RV infarction is reduced LV preload, which causes reduced cardiac output/shock and hypotension.
Avoid therapies that further reduce preload (nitrates, narcotics, propofol, etc.)
Use therapies to improve preload (IV fluids, vasopressors)
Dobutamine
Improves RV stroke volume, and improves RV afterload by reducing pulmonary vascular resistance
Ideally used after revascularization, as inotropes can cause complications during acute MI (arrhythmias, increase in infarct size, etc.)
Heart Block
Inferior infarct-related heart block:
Usually RCA, rarely can be circumflex
Heart block associated with high-vagal tone Bezold-Jarisch reflex or rarely from AV node ischemia
Often transient and can be treated with atropine
Pacemaker should generally be avoided due to risk of RV perforation (can be placed in extreme circumstances)
Anterior infarct-related heart block:
Usually related to extensive infarct and damage to the conduction system in the septum
Complete heart block often preceded by RBBB + LAFB
Temporary/permanent pacemaker more likely to be required; usually see more distal conduction disease like Mobitz 2, third degree heart block, or alternating bundle branch blocks
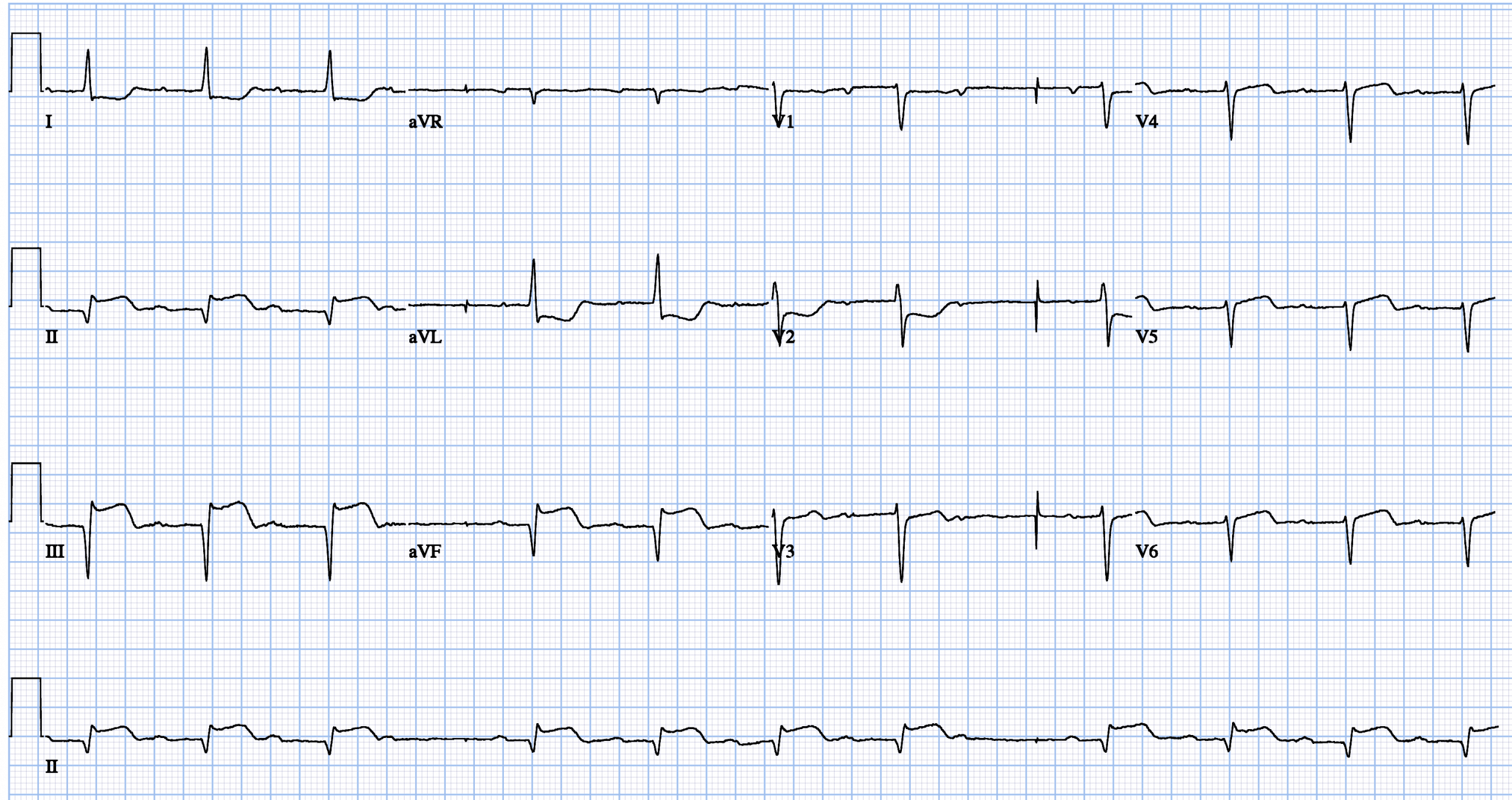
Inferior STEMI with Wenkebach
Ventricular Septal Defect
A very uncommon complication of acute MI.
Typically seen in late-presenting patients who have not been revascularized. They are often female, older patients, and have no history of MI/Angina prior to presentation (less collaterals).
Often have poor prognosis.
Types
Anterior Infarct often located at the apical ventricular septal.
Inferior Infarct often located at the inferobasal ventricular septum. Usually a worse prognosis.
Clinical Features
Prominent pan-systolic murmur at left lower sternal border often associated with a thrill.
Signs of right sided heart failure, pulmonary edema or shock.
Echo helps confirm evidence of a VSD with left to right shunt as well as complications such as RV failure.
Apical 4 Chamber
Apical 4 color
TEE 4 chamber view. Note the dilated RV.
Colour doppler over the ventricular septum does not reveal VSD but turbulent flow suggestive.
2 Chamber view confirms inferior akinesis and thin myocardium.
Gastric view of the ventricular septum with evidence of drop out.
Colour doppler confirms flow accross the ventricular septum.
Management
Hemodynamic support with ionotropes, afterload reduction with nitroprusside and can consider IABP for mechanical support as bridge to surgery
Surgical closure or percutaneous options
Myocardial Rupture
Uncommon complication but very high mortality.
The risk factors are similar to VSDs: patients are often older, late-presenting, female, first presentation MI (lack of collaterals)
Patients can have sudden PEA arrest from cardiac tamponade
Myocardial rupture is typically preceded by pain similar to the patient’s initial presentation
Hypertension, excessive straining, coughing, or vomiting may be triggers
Parasternal long axis, note the possible pericardial effusion.
Apical 4, note the RA inversion a sign of hemodynamic compromise from effusion.
Apical 2, note the inferior wall hypokinesis suggesting inferior infarct.
Apical 3, showing circumfrential effusion.
Subcostal view demonstrating complex effusion with hematoma.
Subcostal view demonstrating complex effusion with hematoma.
Subcostal view of the IVC, showing lack of collapse this suggest high atrial pressures.
Doppler over the apex to try and visualize flow into the pericardium.
Management
Cardiac Arrest → Standard ACLS plus pericardiocentesis
Traditionally, pericardiocentesis was discouraged in patients with myocardial rupture due to concern of worsening hemorrhage into the pericardial space. However, pericardiocentesis (with removal of only 10-50 mL) is still sometimes performed in patients with extreme hemodynamic instability to improve hemodynamics until definitive surgical management is delivered.
Surgical consultation is a must. Teflon or pericardial patch can be performed on the epicardium to stabilize the rupture.
Papillary Muscle Rupture
Presentation:
Acute severe pulmonary edema
Hypotension
Shock
Murmur: may not be very loud because of rapid equalization of pressures across the mitral valve, but patients will have severe MR
Posteromedial papillary muscle
Most common
Single blood supply PDA
Anterolateral papillary muscle
Dual blood supply from the LAD and circumflex artery
Physical Exam / POC-US:
Patients often have a hyperdynamic LV because severe MR reduces LV afterload, by allowing blood to pass to a low-pressure left atrium. This paradoxically improves LV systolic function, and it often becomes hyperdynamic (EF > 70%).
Patients with acute MR develop acute severe pulmonary edema (“Flash pulmonary edema”) – they are acutely dyspneic requiring high O2.
Physical exam will reveal acute congestion (pulmonary edema), and poor forward flow (cyanosis, pallor, confusion, lethargy, poor capillary refill).
S3 “gallop” heart sound is very commonly auscultated, and is a classic finding.
A murmur is very uncommon in severe MR because regurgitant flow is laminar across a wide-open mitral valve. Murmurs are produced by turbulent flow.
Treatment
Acute Stabilization:
Afterload reduction (if blood pressure allows)
Reducing afterload facilitates forward flow into aorta, and reduces regurgitation (often target MAP 60-65mmHg). However, the patient is often in shock and hypotensive, which precludes the use of vasodilators for afterload reduction. Afterload reduction to reduce MR must be balanced against severe hypotension, which reduces organ/coronary perfusion.
Inotropes
May need to combine with vasopressors to avoid severe hypotension.
Inotropes may temporize the situation, but are unlikely to independently rescue a patient with acute MR.
IABP
Excellent solution to reduce afterload, and facilitate forward flow.
IABP insertion is the best step to temporize a patient with acute severe MR.
URGENT surgical consult
Patients with acute severe ischemic MR will not survive without EARLY surgical intervention.
Cardiac surgery must be consulted WITHOUT DELAY.
Transthoractic Echo
PLAx View
PLAx view Color
Parasternal Short Axis – Mitral Level
Apical 4 Chamber
Transesophageal Echo
Gastric View on TEE demonstrating pap muscle rupture.
Gastric View on TEE demonstrating pap muscle rupture.