| Ball-in-Cage | Single Tilting Disk | Bi-leaflet Tilting Disk | New Generation Bi-leaflet Tilting Disk |
|---|---|---|---|
 | 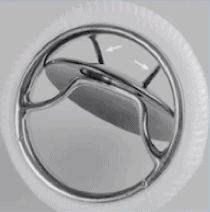 | 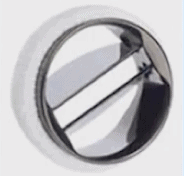 |  |
| Starr-Edwards | Bjork-Shiley | Medtronic bileaflet | On-X Valve |
|
|
|
|
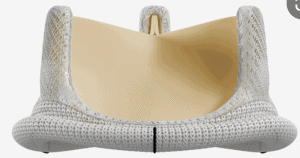
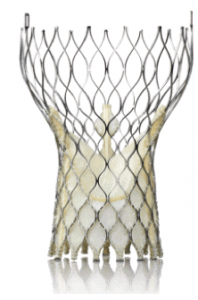
| Surgical Valves | Transcatheter Self-Expanding (TAVR) | Transcatheter Balloon Expandable (TAVR) |
|---|---|---|
 |  |  |
|
|
|
| Ball-in-Cage | Single Tilting Disk | Bi-leaflet Tilting Disk | New Generation Bi-leaflet Tilting Disk |
|---|---|---|---|
| | | |
| Starr-Edwards | Bjork-Shiley | Medtronic bileaflet | On-X Valve |
|
|
|
|
| Surgical Valves | Transcatheter Self-Expanding (TAVR) | Transcatheter Balloon Expandable (TAVR) |
|---|---|---|
| | |
|
|
|