- Patients should remain on dual antiplatelet therapy post-MI
- ASA, ticagrelor, clopidogrel, and prasugrel all have mortality benefit post-MI
- Optimal duration:
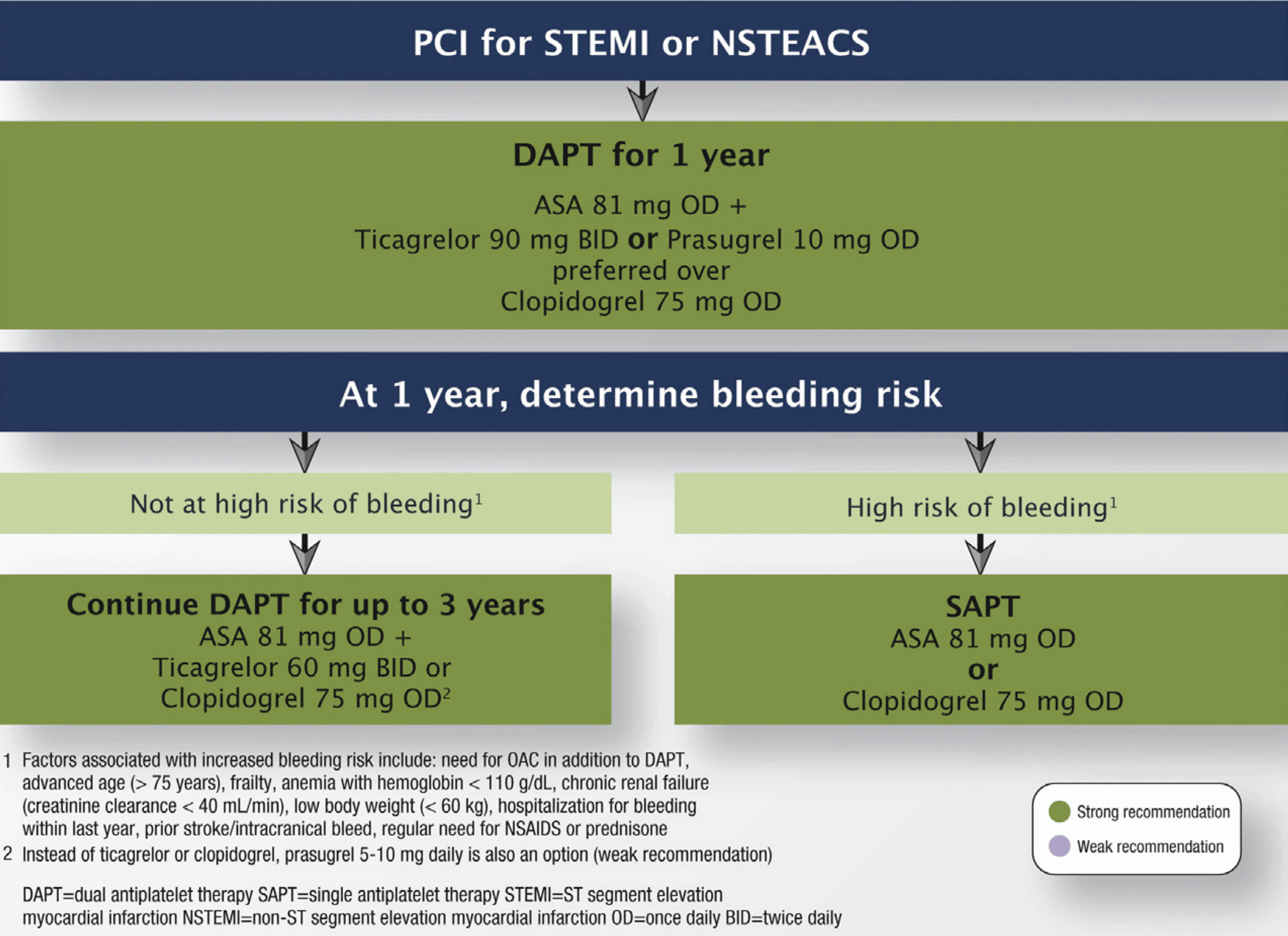
- STEMI or NSTEMI: At least 1 year (CCS)
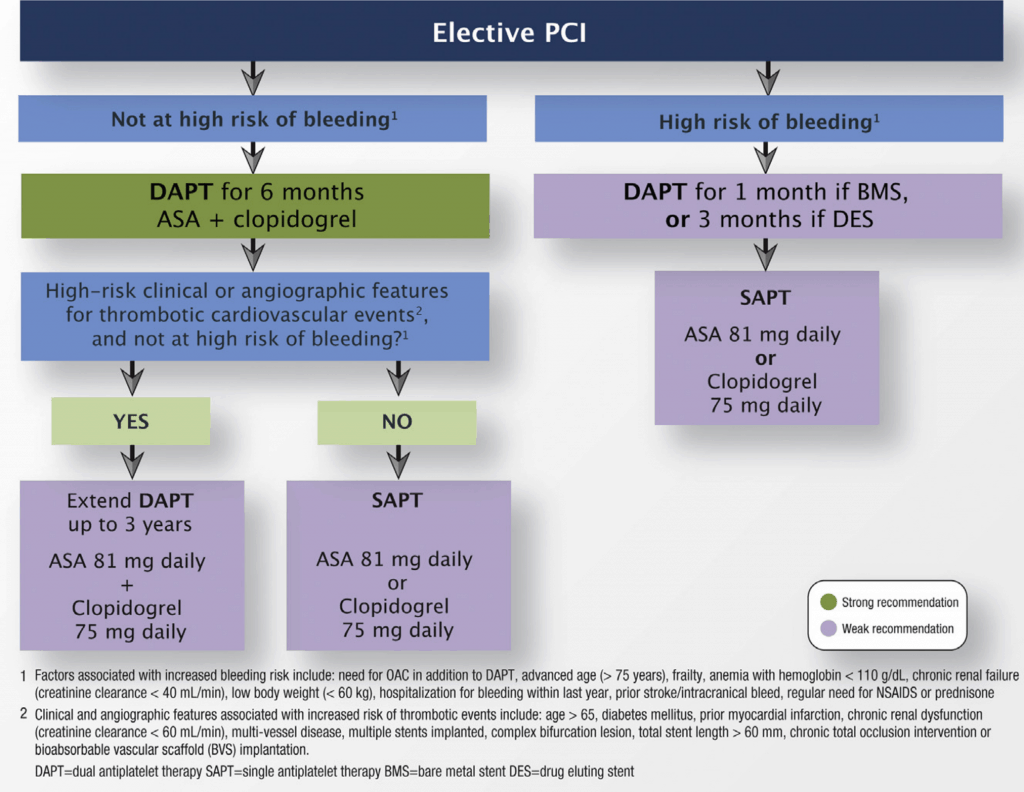
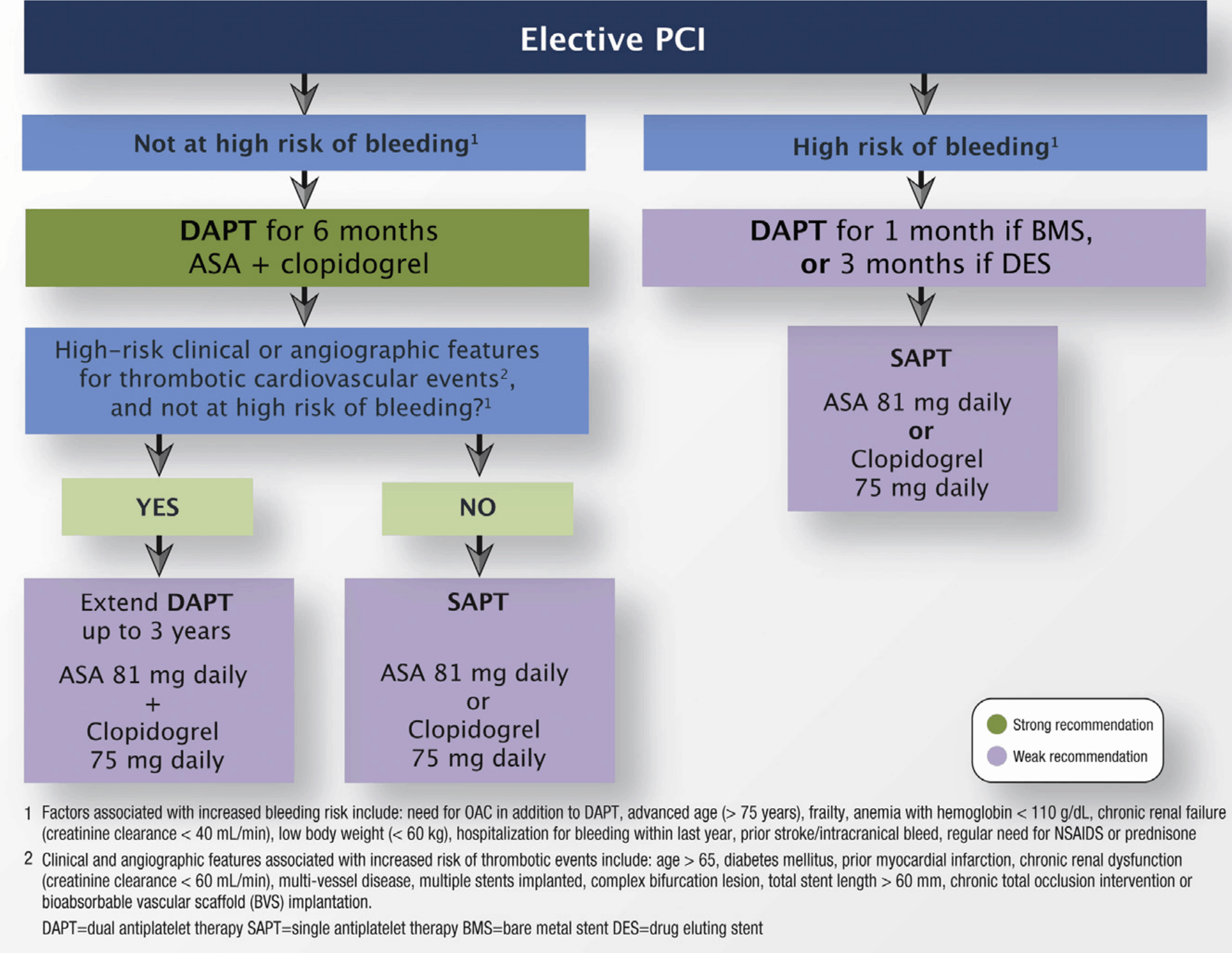
CCS 2018 – Recommendations for duration of DAPT in patients who undergo elective PCI - Elective PCI (Outpatient): At least 6mo (CCS)
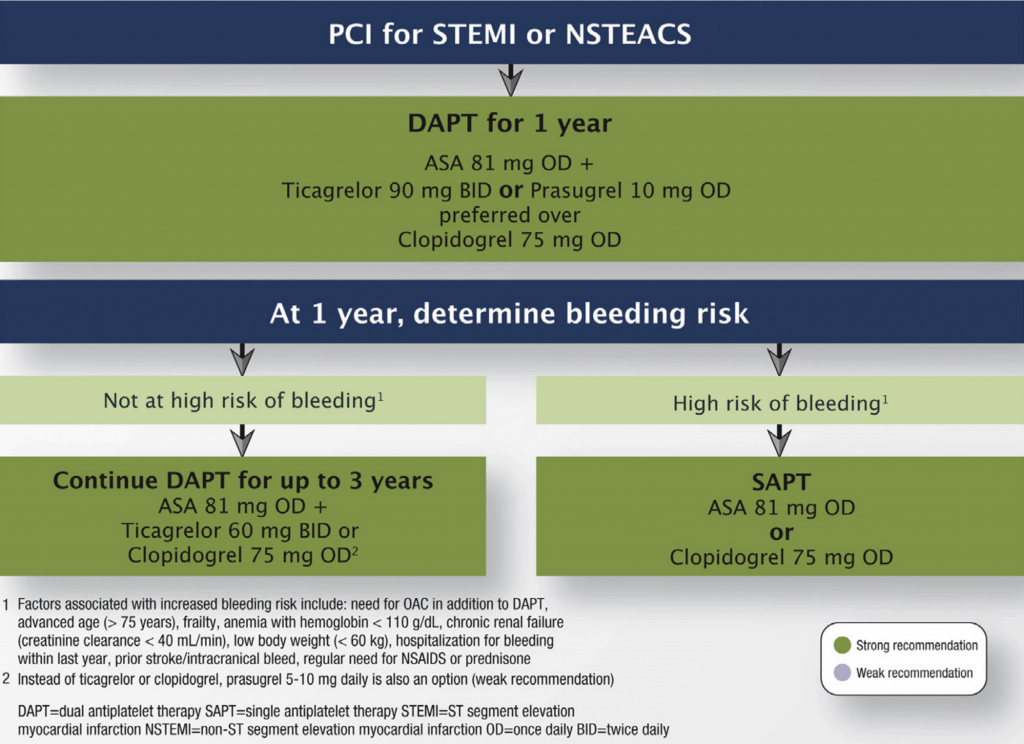
CCS 2018 – Recommendations for duration of DAPT in patients with ACS (STEMI or NSTEACS) who undergo PCI - There is evidence to continue >1 year
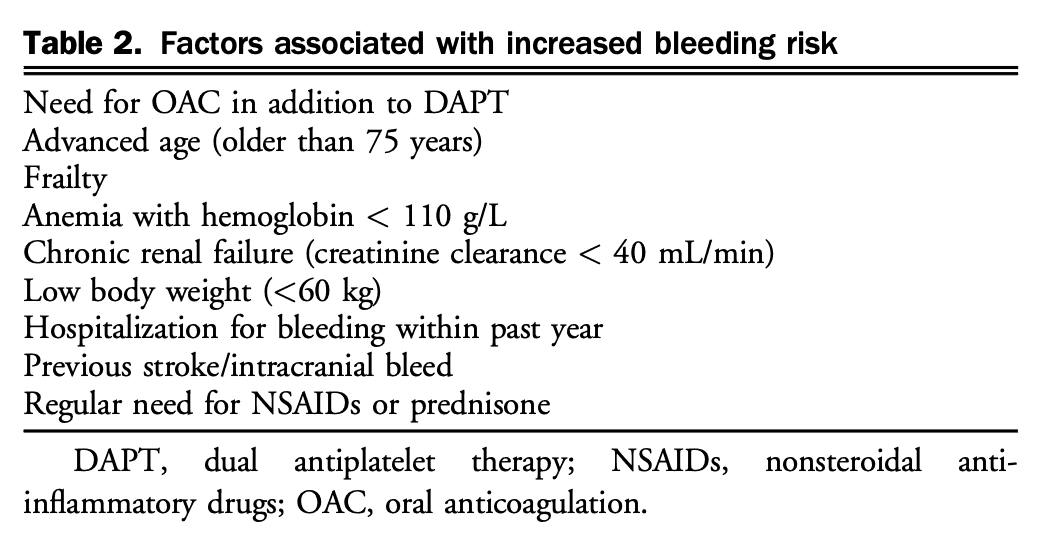
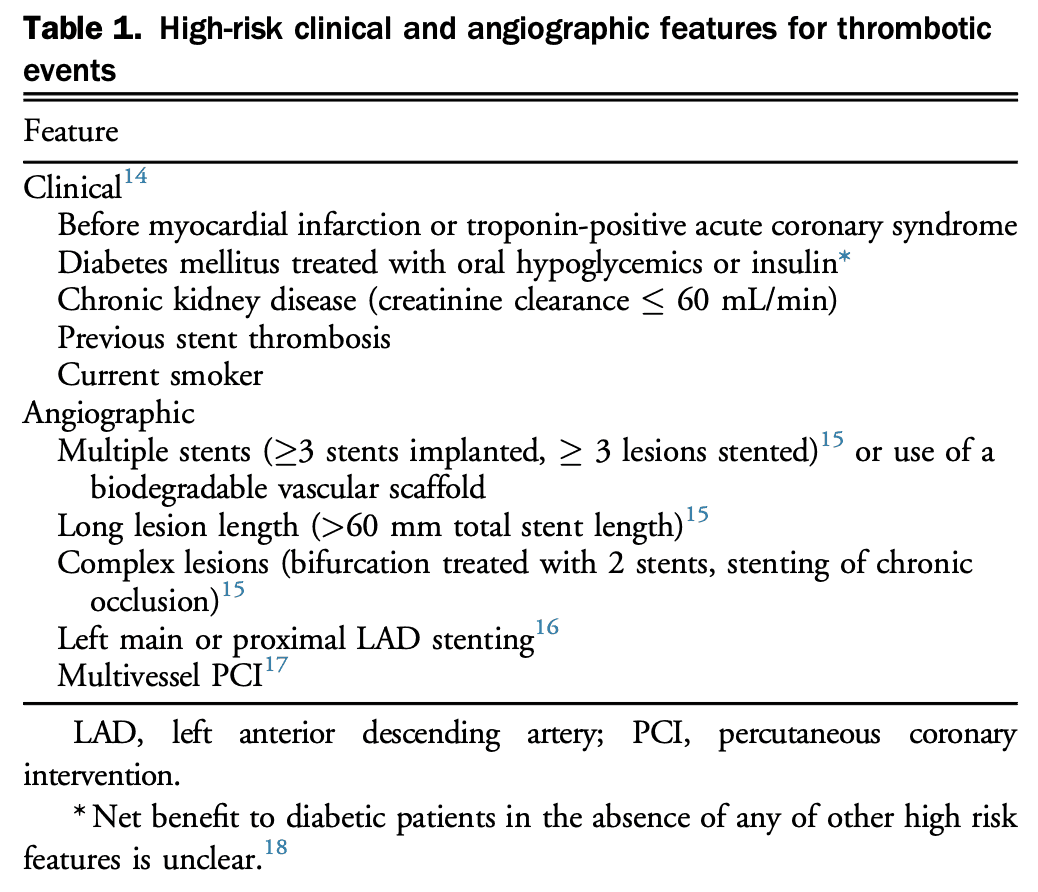
- At 1 year, weigh risks of bleeding vs. risk of ischemic events (See Table to the right)
- Generally, if tolerating DAPT at 1 year post-MI, continue for up to 3 years with one of the following proven regimens:
- ASA 81 mg daily + ticagrelor 60 mg BID (REDUCED DOSE) (PEGASUS-TIMI-54 Trial)
- ASA 81 mg daily + clopidogrel 75 mg daily (DAPT Trial)
- ASA 81 mg daily + prasugrel 10 mg daily (DAPT Trial) – not available in Canada
- STEMI or NSTEMI: At least 1 year
Beta Blockers
- Indications: Start within 24 hours of ACS diagnosis (unless contraindication), continue for at least 3 years [Class I]
- Benefits: Reduce ischemia, re-infarction, arrhythmias, mortality.
- Acutely in MI: Benefits controversial, more benefit in chronic post-MI care
- Trials: TIMI-2B Study, BHAT (mortality benefit), COMMIT (no benefit), (N Engl J Med. 1983; 308:614–8)
- Options/Doses:
- If no LV dysfunction (post-MI prevention): Metoprolol 12.5 mg BID, atenolol 12.5-25 mg OD, benefit extrapolated to bisoprolol 2.5 mg OD
- If LV dysfunction: Bisoprolol 2.5 mg daily, carvedilol 3.125 mg BID, metoprolol 12.5 mg BID
- If contraindicated: Re-evaluate in 24 hours
- Contraindications: (if contraindicated, re-evaluate in 24hrs)
- Acute heart failure (risk of precipitating cardiogenic shock)
- Evidence of low-output state / cardiogenic shock
- AV block: 3rd/2nd degree, PR interval > 240ms
- Severe asthma/COPD
ACE Inhibitors
(use ARB if ACEi-intolerant)
- Indications: Proven benefit in post-ACS patients with ANY of: EF < 40%, HTN, DMII, or CKD [Class I], but benefit extrapolated to all ACS within 24hrs [Class IIB]
- Trials: SAVE, AIRE, HOPE
- Options/Doses:
- Ramipril 2.5-5 mg OD (titrate to 10 daily – AIRE study)
- Perindopril 2 mg OD (titrate to 8 mg – PREAMI study)
- Enalapril (CONSENSUS II – no benefit)
- Indications: Proven benefit in post-ACS patients with ANY of: EF < 40%, HTN, DMII, or CKD [Class I], but benefit extrapolated to all ACS within 24hrs [Class IIB]
Mineralocorticoid Receptor Antagonists (MRA)
- Indications:
- Need all of: On max dose ACEi, BB, and post-MI + EF ≤ 40% + (HF symptoms or DMII) [Class I]
- CCS 2017 HF Guideline: “MRA for patients with acute MI with EF < 40% and HF or with acute MI and an EF < 30% alone in the presence of diabetes”
- Trial: EPHESUS
- Need all of: On max dose ACEi, BB, and post-MI + EF ≤ 40% + (HF symptoms or DMII) [Class I]
- Options/Doses:
- Eplerenone 25 mg daily (titrate up to 50 mg daily)
- Contraindications (for post-MI indication):
- Creatinine > 221 (men), > 176 (women)
- K+ > 5.0
- Indications:
- Calcium channel blockers (diltiazem/verapamil)
- 2nd line to beta blockers (if ongoing ischemia), reduce re-infarction
- Negative inotropes → contraindicated in LV dysfunction
- Indicated for coronary artery spasm
High-Intensity Statins
- Indications: All ACS patients [Class I]
- Benefits: Reduces recurrent MI, CV mortality, need for revascularization, and stroke
- Trials: PROVE IT-TIMI 22, MIRACL, TNT (high dose)
- Options/Doses:
- Atorvastatin 40-80 mg
- Rosuvastatin 20-40 mg
- Pravastatin and simvastatin are not high-intensity statins.
- ESC 2017 STEMI recommendations for post-MI care
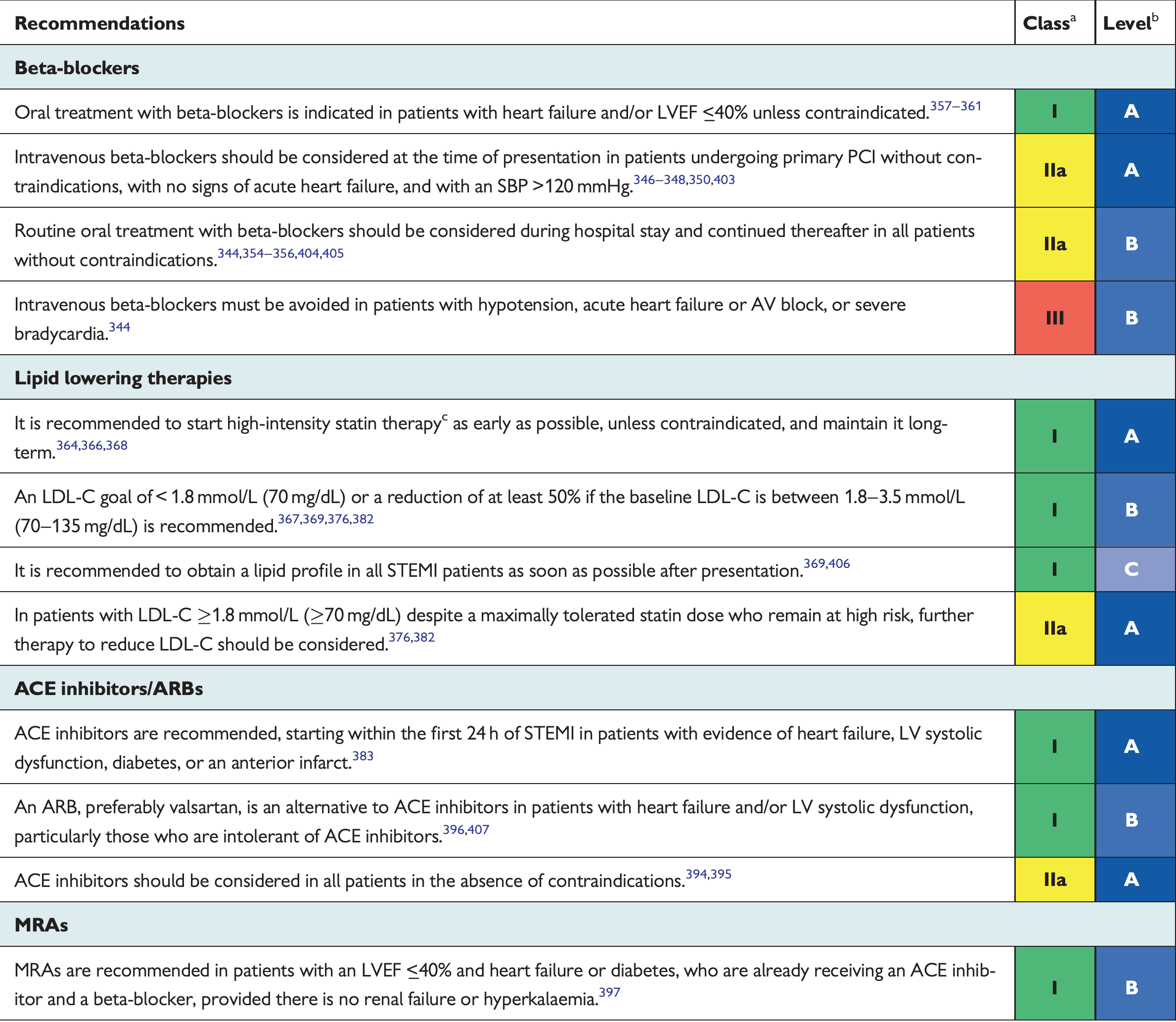
2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation - NOTES:
- NSAIDs contraindicated post-MI (increases risk of MACE)
- All admitted NSTEMI patients need 24 hours of rhythm monitoring (or until revascularization), and only select UA patients
- STATIN-indicated conditions: (conditions that require statin use as per CCS 2021 Lipid Guidelines)
- LDL ≥ 5.0 mmol/L
- Most patients with diabetes (Age ≥ 40 or ≥ 30 and ≥ 15y of DM duration)
- ASCVD (MI/ACS, Stable Angina, coronary artery disease, Stroke, TIA, PAD, AAA)

{kind=link}
{kind=link}
{kind=link}