- Left main coronary artery (LMCA) arises from right sinus of Valsalva, either directly from right coronary artery or as a separate ostia
- LMCA course anterior to pulmonary artery (anterior) (c)
- LMCA course posterior to aorta (posterior) (d)
- LMCA course intramyocardial (subpulmonic/transeptal) (e)
- LMCA course between aorta and pulmonary artery (interarterial) (f)
- Left anterior descending coronary or left circumflex coronary artery may originate from the right sinus alone
- Right coronary artery (RCA) arises from left sinus of Valsalva, either from LMCA or as a separate ostia
- RCA courses anterior to pulmonary artery (anterior)
- RCA courses posterior to aorta (posterior) (b)
- RCA courses between aorta and pulmonary artery (interarterial) (g)
- Single LMCA arises from left sinus of Valsalva and bifurcates into the left anterior descending coronary and left circumflex coronary arteries. The left circumflex coronary artery crosses the crux and continues as the RCA.
- Single RCA arises from right sinus, crosses crux, continues as left anterior descending coronary and left circumflex coronary arteries
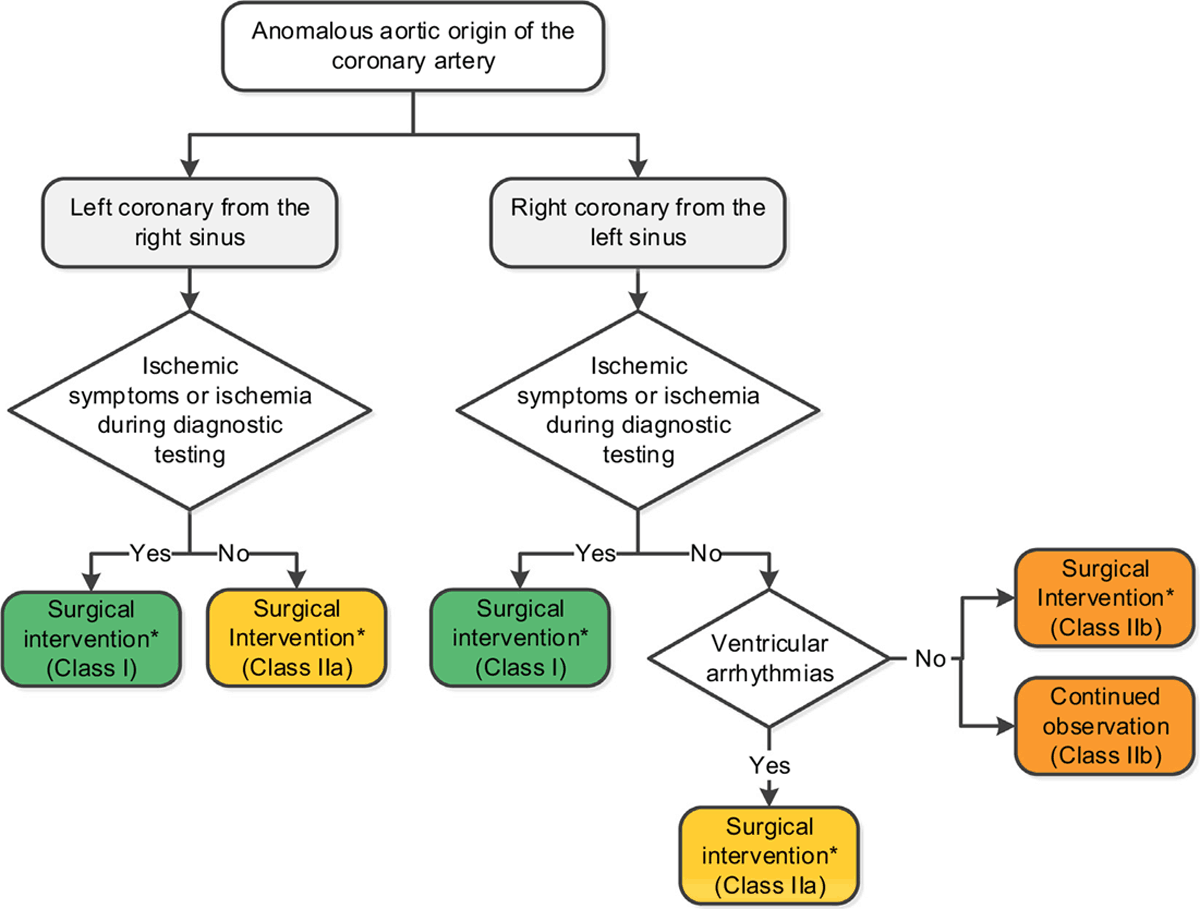
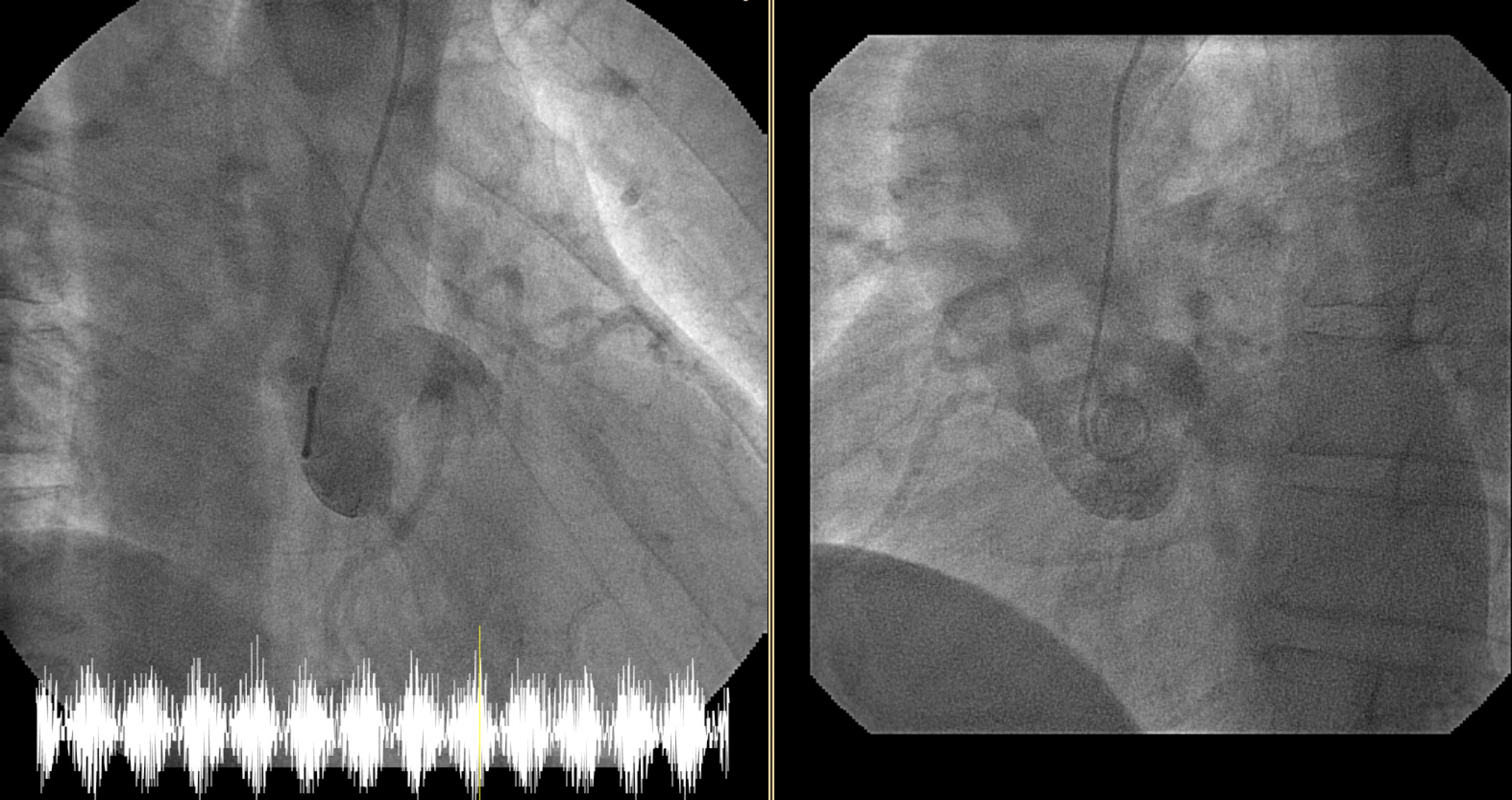
ATS 2017: Expert consensus guidelines: Anomalous aortic origin of a coronary artery