A defect in the ventricular septum resulting in a communication between the right and left ventricle.
Common congenital abnormality which occasionally requires surgical intervention.
Can occur after a myocardial infarction usually to patients presenting late to hospital.
Classically the smaller the VSD the louder the heart murmur usually best heart at the left lower sternal border and is pansystolic.
Types of VSD
Subarterial: Least common and associated with aortic insufficiency due to close proximity to the aortic valve.
Membranous: Most common type of VSD involving the membranous septum and accounting for usually 80% of cases.
AV canal type.
Muscular: Second most common type and most likely to close spontaneously.
Characteristics
Often characterized as Restrictive vs non-restrictive and based on the size small, medium and large.
In Restrictive VSD’s the LV pressure is higher than the RV.
In non-restrictive RV and LV have similar pressures.
Example 1 Muscular VSD
Parasternal views demonstrating flow accross the ventricular septum.
Apical 4 chamber view demonstrating a clear defect in the septum and colour doppler confirms left to right blood shunting.
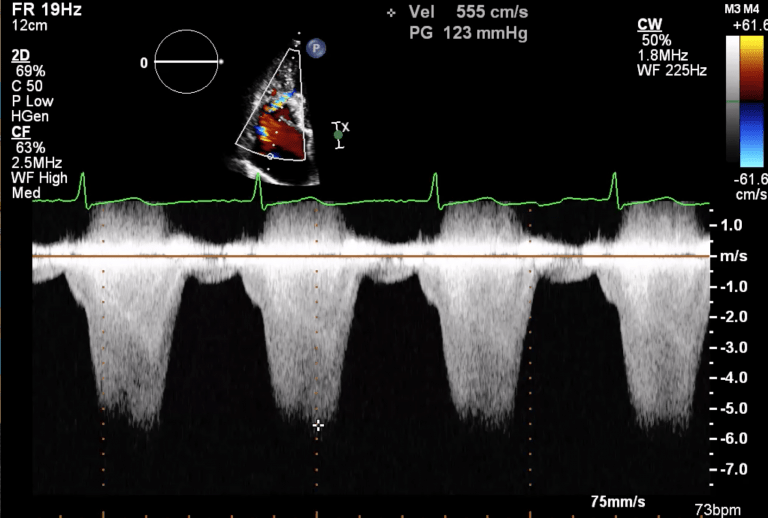
Continuous wave doppler across the VSD demonstrating the peak gradient.
Example 2 Membranous VSD
Parasternal long axis view showing evidence of a membranous VSD. Note the colour flow just below the aortic valve, this is the common location for membranous VSD.
There is also trace aortic regurgitation.
Short axis view at the level of the aortic valve demonstrating colour flow into the right ventricle.
Zoomed apical 5 chamber demonstrating colour flow across the ventricular septum consistent with a membranous VSD.