Please see original article: Syncope for full details on the differential and diagnostic approach to syncope
Details regarding pacing will be discussed in other topics, a general overview of indications for pacing in patients with cardiac syncope will be outlined below.
Bradycardia related syncope
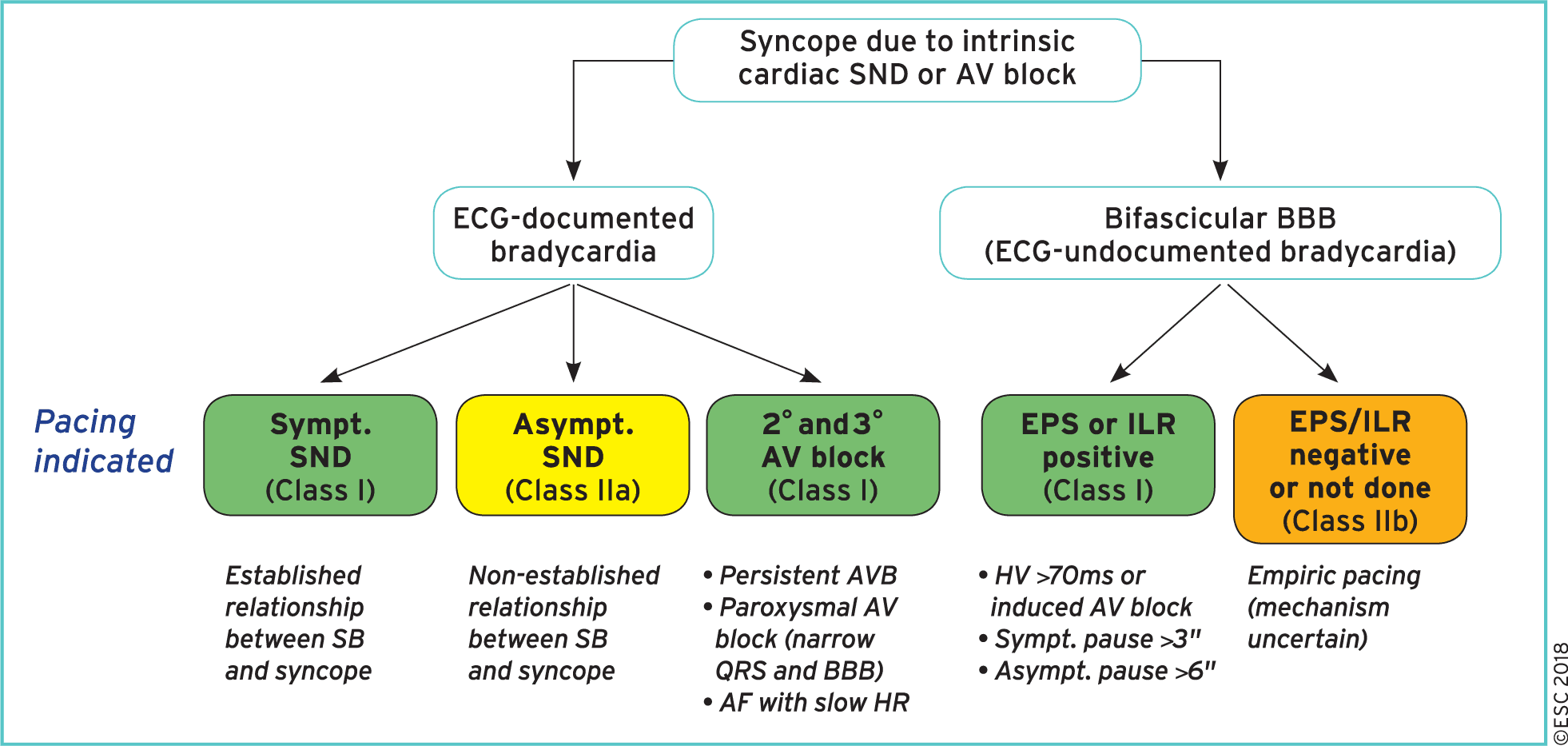
Cardiac pacing is indicated when there is an established relationship between syncope and symptomatic bradycardia due to (Class I):
Sick sinus syndrome
Intrinsic AV block
Cardiac pacing is indicated in intermittent/paroxysmal intrinsic third- or second-degree AV block (including AF with slow ventricular conduction), although there is no documentation of a correlation between symptoms and ECGs (Class I).
Cardiac pacing should be considered when the relationship between syncope and asymptomatic sinus node dysfunction is less established (Class IIa)
Summary of indications for pacing in patients with syncope due to intrinsic cardiac bradycardia
Bifascicular Bundle Branch Block
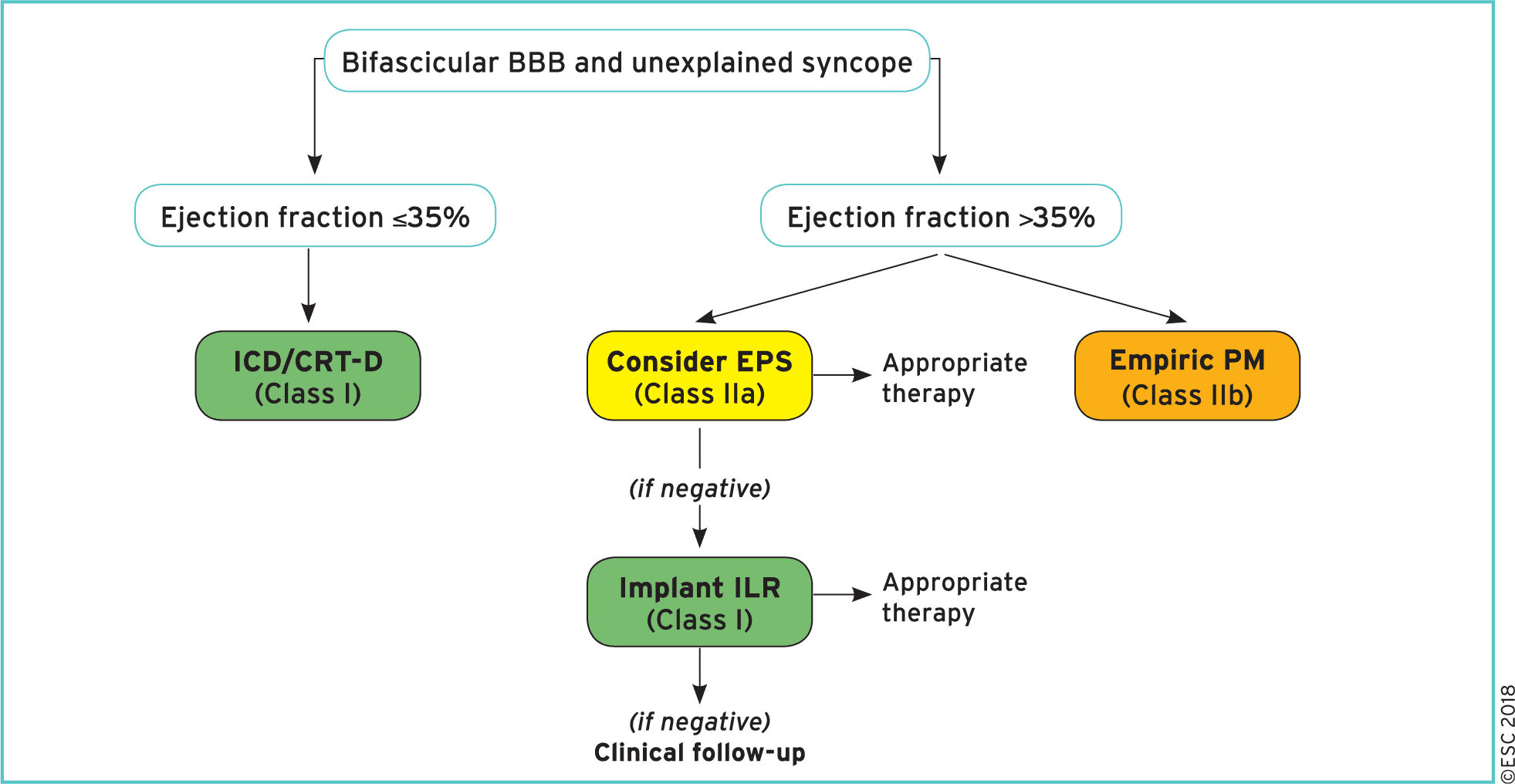
Pacing indicated in patient with syncope, bundle branch block and documented AV block AV block on loop recorder or positive electrophysiology study (Class I)
Therapeutic algorithm for patients presenting with unexplained syncope and bundle branch block.
Tachycardia related syncope
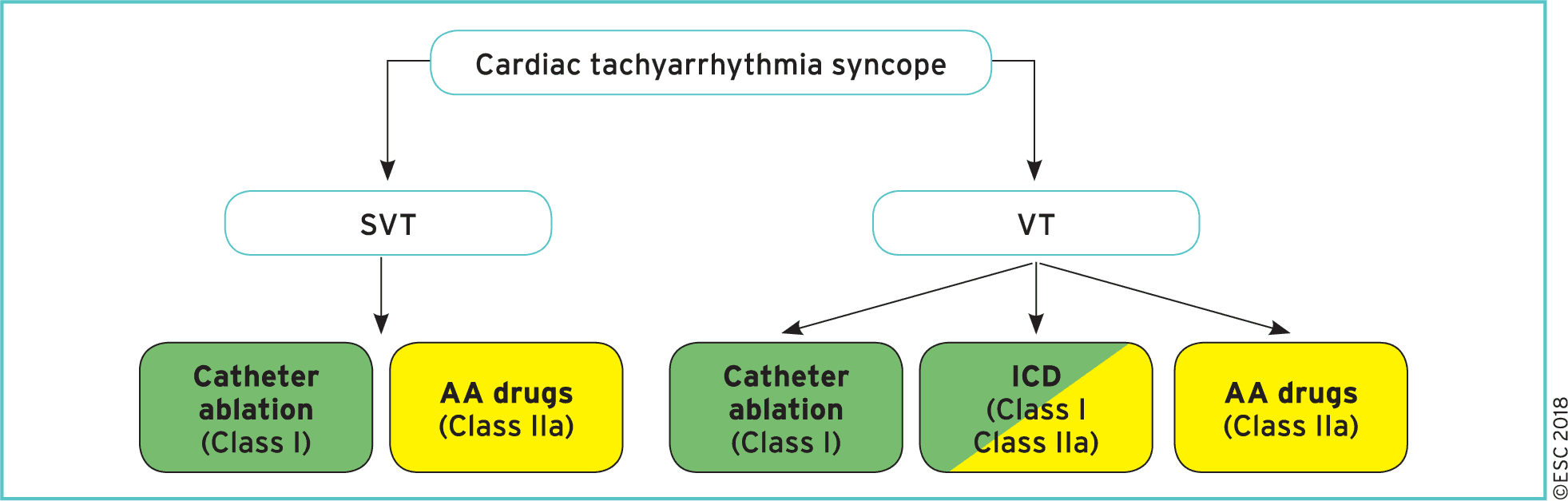
Catheter ablation is indicated in patients with syncope due to SVT or VT in order to prevent syncope recurrence. (Class I)
An ICD is indicated in patients with syncope due to VT and an ejection fraction <35% (Class I)
An ICD is indicated in patients with syncope and previous myocardial infarction who have VT induced during EPS (Class I)
An ICD should be considered in patients with an ejection fraction >35% with recurrent syncope due to VT when catheter ablation and pharmacological therapy have failed or could not be performed. (Class IIa)
Antiarrhythmic drug therapy, including rate-control drugs, should be considered in patients with syncope due to SVT or VT. (Class IIa)
Choice of therapy for patients presenting with syncope due to cardiac tachyarrhythmias as the primary cause
Structural Causes
Syncope in patients with structural heart disease or inheritable arrhythmia syndromes is associated with a two- to four-fold increased risk of death!
Implantable cardioverter defibrillator indications in patients with unexplained syncope and left ventricular systolic dysfunction:
ICD therapy is recommended to reduce SCD in patients with symptomatic heart failure (NYHA class II–III) and LVEF <35% after >3 months of optimal medical therapy, who are expected to survive >1 year with good functional status.(Class I)
ICD should be considered in patients with unexplained syncope with systolic impairment, but without a current indication for ICD, to reduce the risk of sudden death (Class IIa)
Implantable loop recorder (instead of ICD) may be considered in patients with recurrent episodes of unexplained syncope with systolic impairment, but without a current indication for ICD. (Class IIb)
Topics of Hypertrophic cardiomyopathy, Arrhythmogenic right ventricular cardiomyopathy, Long QT syndrome will be discussed separately.
Further Reading
2018 ESC Guidelines for the diagnosis and management of syncope (html) (pdf)
Authors
Primary Author: Dr. Dimitar Saveski (MD, FRCPC, Internal Medicine Resident)